





Pearl-like mass on a girl’s tympanic membrane
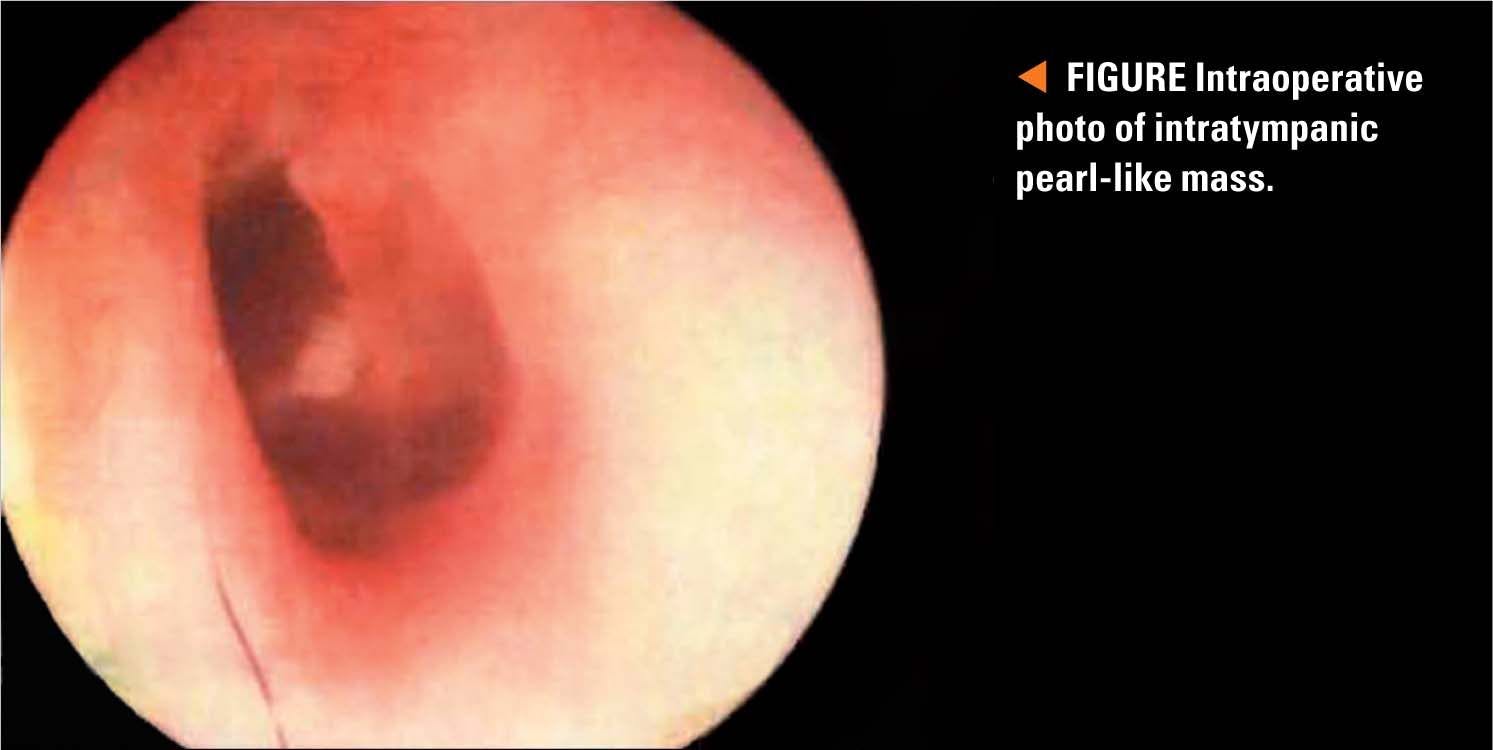
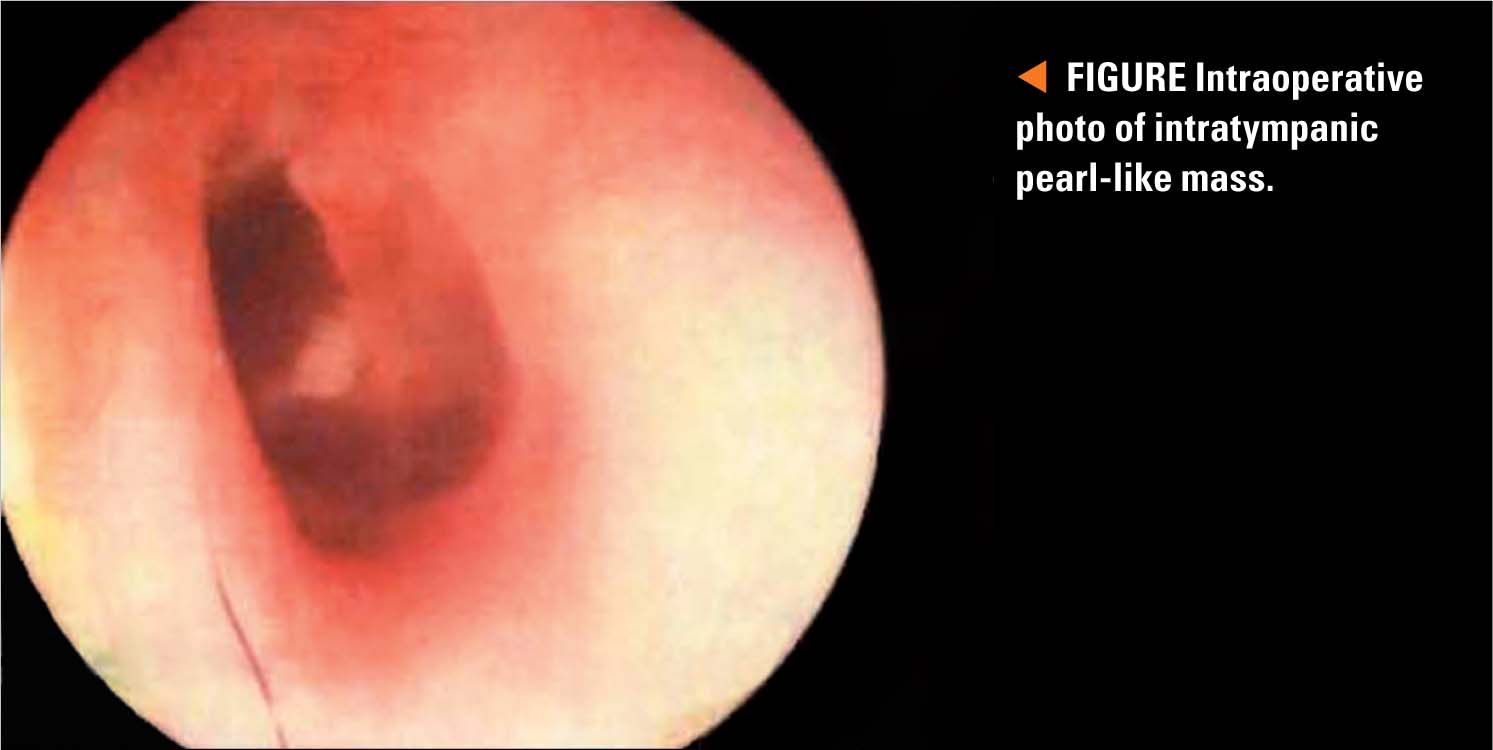
During a routine office visit for mild acute nasal congestion and possible diminished hearing, an isolated, small, pearl-like mass was noted just posterior to the umbo of the left tympanic membrane of a 5-year-old girl.

The Case
During a routine office visit for mild acute nasal congestion and possible diminished hearing, an isolated, small, pearl-like mass was noted just posterior to the umbo of the left tympanic membrane (TM) of a 5-year-old girl (Figure). She was otherwise well. There was no history of traumatic perforation of the tympanic membrane or otorrhea.
NEXT: What's the diagnosis?
History
At a follow-up visit 2 months later, the same lesion was still visible. An office screening audiogram was performed and the child easily passed without any deficits at the 20 dB screening threshold.
The girl had had tympanostomy tubes inserted 3 years ago because of 4 episodes of acute otitis media in the previous 12-month period. The tympanostomy tubes had remained in place for about 18 months, and then extruded spontaneously.
Differential diagnosis
The most common white lesion on the TMs of young children is a calcified tympanosclerotic plaque (Table 1). Recall that the child had had tympanostomy tubes inserted several years prior and that the tubes had remained in place for more than 1 year.

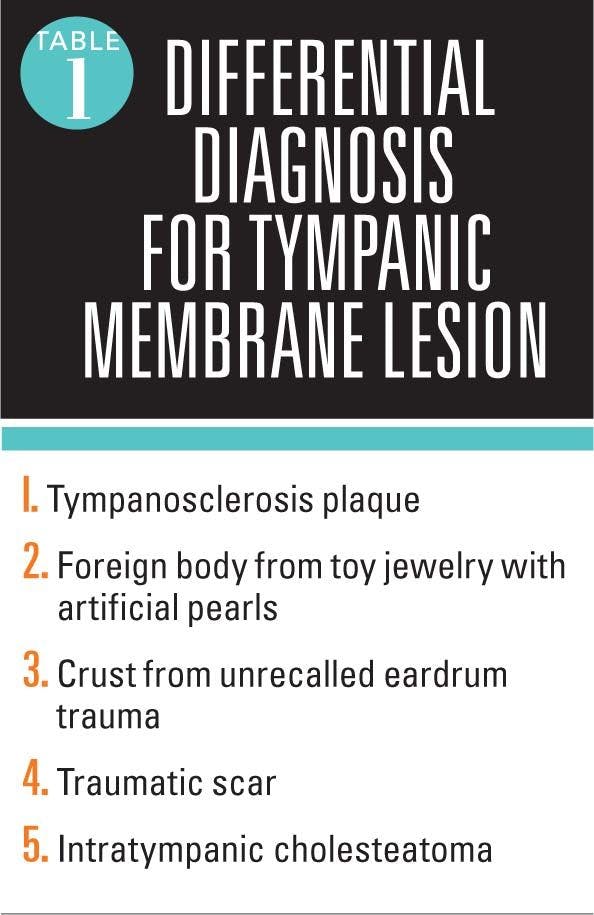
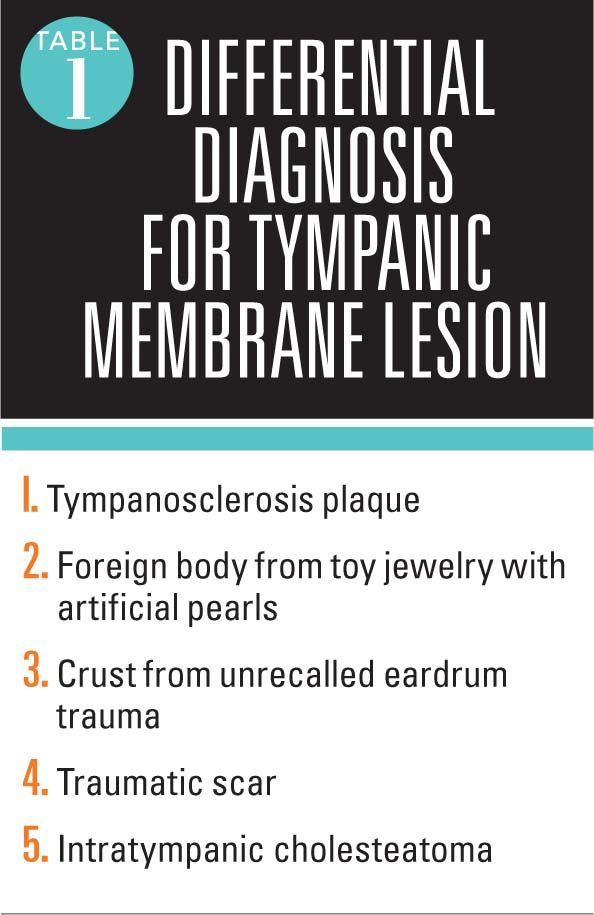
The most common misdiagnosis of an intratympanic cholesteatoma is tympanosclerosis. Additional diagnostic considerations include desquamation of all or part of the tympanic membrane. This can occur during the recovery phase of acute otitis media caused by the more virulent Streptococcus pyogenes or Streptococcus pneumoniae. The pearl-like lesion also could possibly be a real foreign body such as a toy pearl, bead, or Styrofoam pellet that was stuck on the center of the TM.
Physical examination with otomicroscopy
Examination of the left tympanic membrane with otomicroscopic magnification at the otolaryngologist’s office revealed a glistening, tiny, 3-dimensional round cystic lesion pointing toward the ear canal. It was clearly separated from the middle fibrous layer of the TM, thus ruling out a tympanosclerosis scar.
More: Why otitis media prevalence is decreasing
The patient was referred to a pediatric otolaryngologist who made a definitive diagnosis of intratympanic pearl-like cholesteatoma.
Discussion
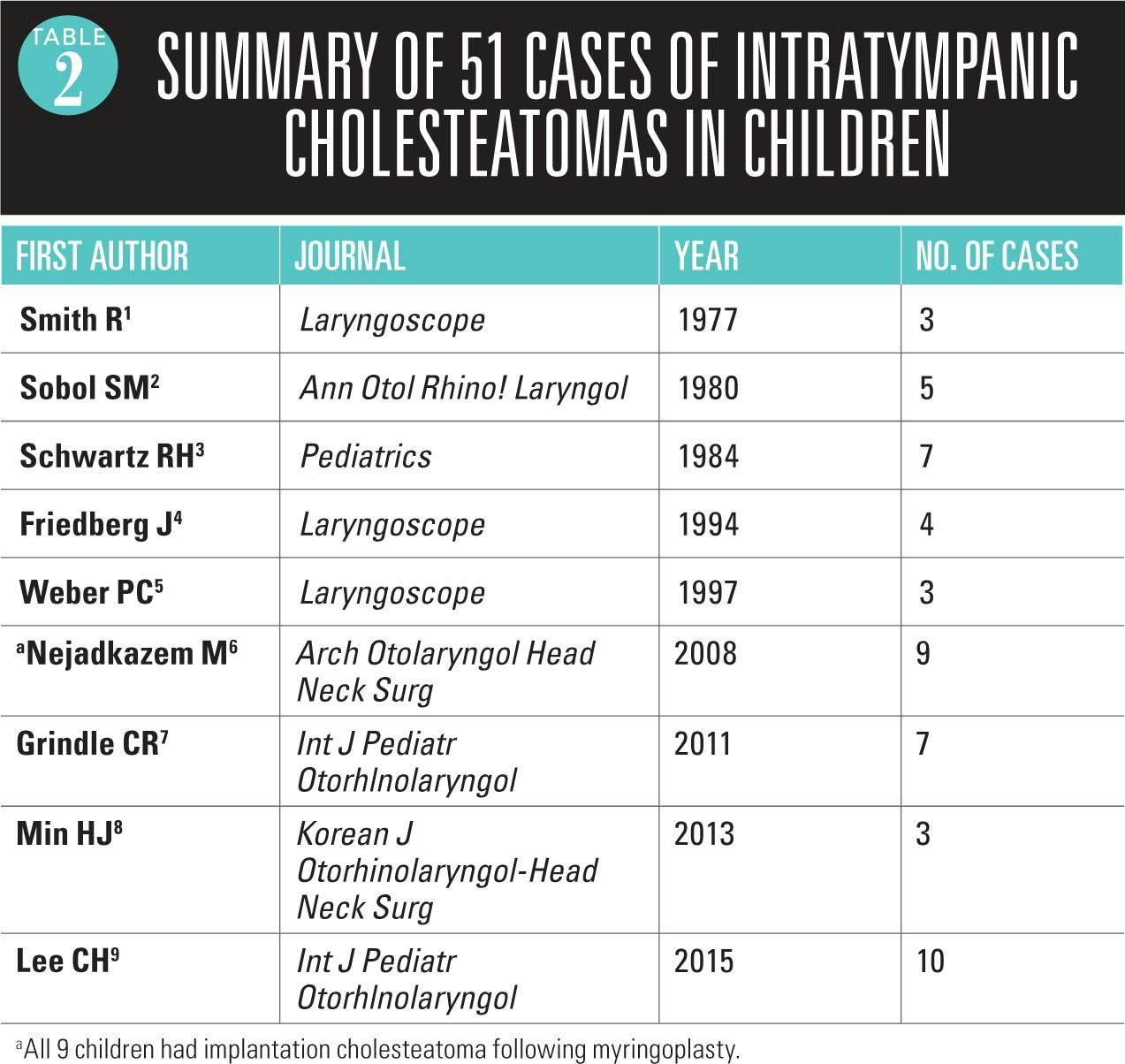
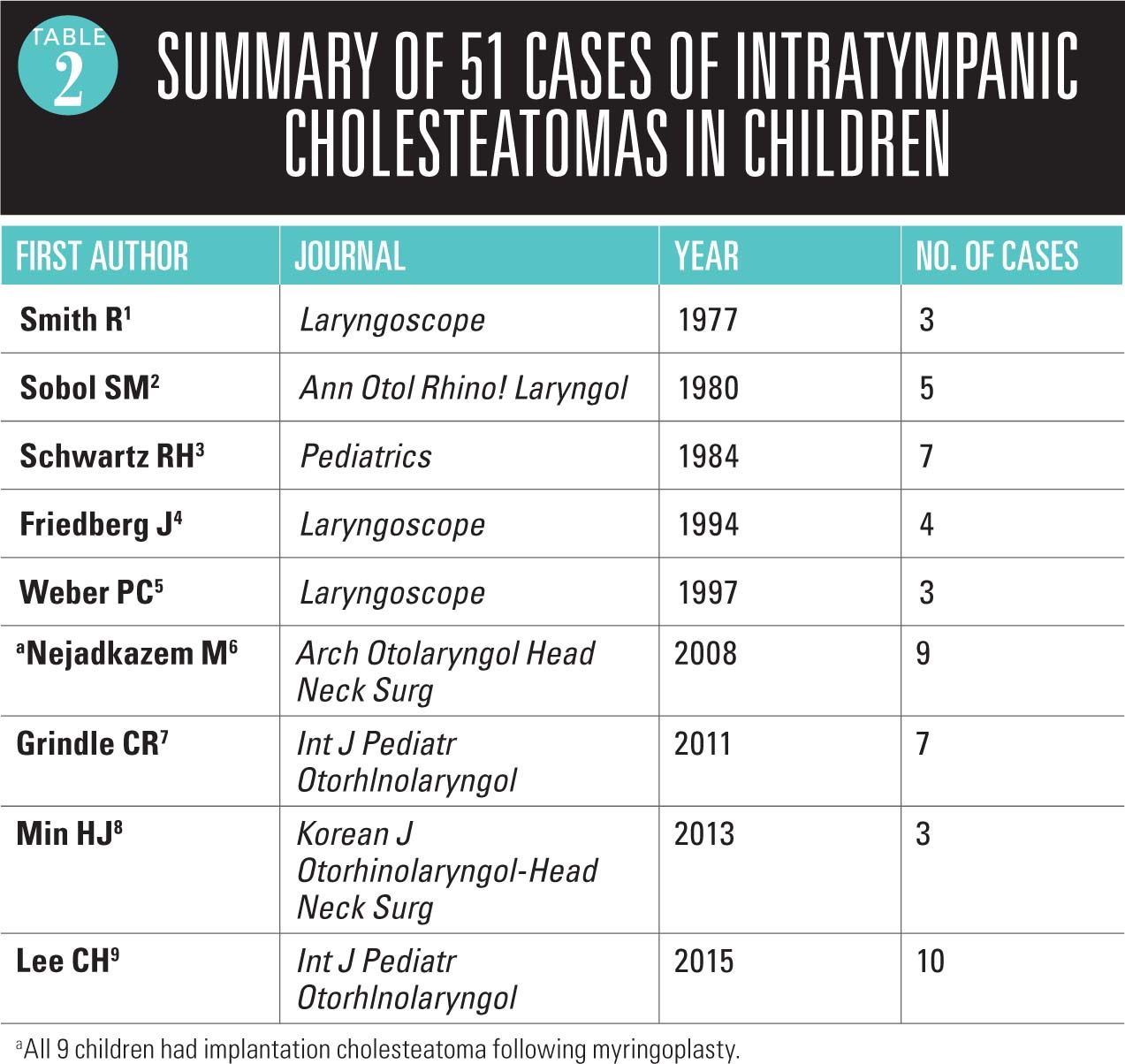
The characteristic location of a congenital middle-ear space cholesteatoma (mesotympanic cholesteatoma) is in the anterior or posterior superior quadrant where it is seen under otoscopic magnification appearing as a white or golden-colored round mass. Primary congenital intratympanic cholesteatomas, characterized by accumulation of keratinous debris in the space between the outer epithelial layer and the middle fibrous layer of the TM, are said to be very rare. However, there are more than 50 cases previously reported in the medical literature (Table 2).1-9

In most cases including this case, an intratympanic cholesteatoma appears as if a tiny lustrous pearl is affixed to the lateral layer of the tympanic membrane. The senior author of this article has detected 5 additional intratympanic cholesteatomas in his 43 years in primary care pediatric practice.4,10 The characteristic location of an intratympanic cholesteatoma is in the center of the tympanic membrane, adjacent to the umbo. In contradistinction, tympanosclerotic scars have an incomplete arc-like peripheral location often starting at 1 o'clock on the TM and ending in a 9 o'clock location.
NEXT: Possible outcomes for unrecognized intratympanic cholesteatoma
There are several possible outcomes of an unrecognized intratympanic cholesteatoma. The cyst may rupture spontaneously. The squamous epithelial cyst wall then shrivels up and is cast into the ear canal.11 A second path of evolution occurs when the lesion enlarges. An unknown percentage of these isolated cholesteatomas can invade the middle ear cleft.12-14 In 1 of the authors’ 4 other cases of this unusual intratympanic cholesteatoma, the tiny cyst was believed to be totally excised by an experienced pediatric otolaryngologist. Six months postoperatively, a planned "look see" intraoperative reexamination of the tympanic membrane and middle-ear space revealed an unexpected mesotympanic (middle-ear space) growth of squamous debris from the invasive intratympanic cholesteatoma. Even though apparent complete excision of the entire intratympanic cyst is performed at the time of initial surgery, serial reexaminations at 6- to 12-month intervals is strongly recommended.
Next: Hearing loss and the pediatrician
Undetected and left alone, the cyst may enlarge and even migrate laterally, into the ear canal, or medially, invading the middle and medial layer to the TM and implanting itself and growing in the middle ear cleft where it can damage the middle ear ossicles and even invade the epitympanic space, gradually expanding and causing damage to the middle ear ossicular chain. A computed tomography scan of the middle ear was not performed for this patient, although CT is frequently ordered to help evaluate the middle ear cleft for mesotympanic extension of a cholesteatoma.
Patient outcome
The patient underwent surgical removal of the intact cyst, and histopathology was confirmed as a cholesteatoma. Follow-up evaluation was scheduled with pediatric otolaryngology 6 months later.
Conclusion
lntratympanic cholesteatomas are rare, with 50 reported in the medical literature. There are very few reports of these invasive cysts in the general pediatric literature. They appear as totally innocent-looking, tiny, pearl-like lesions located adjacent to the umbo of the tympanic membrane. Undetected and left alone, some of them enlarge and migrate into the middle-ear cleft, gradually expanding and causing damage to the middle-ear ossicular chain. If still present after a few months of observation, prompt referral to an otolaryngologist is highly recommended.
REFERENCES
1. Smith R, Moran WB. Tympanic membrane keratoma (cholesteatoma) in children with no prior otologic surgery. Laryngoscope. 1977;87(2):237-245.
2. Sobol SM, Reichert TJ, Faw KD, Stroud MH, Spector GJ, Ogura JH. Intramembranous and mesotympanic cholesteatomas associated with an intact tympanic membrane in children. Ann Otol Rhinol Laryngol. !980;89(4 pt 1):312-317.
3. Schwartz RH, Grundfast KM, Feldman B, Linde RE, Hermansen KL. Cholesteatoma medial to an intact tympanic membrane in 34 young children. Pediatrics. 1984;74(2):236-240.
4. Friedberg J. Congenital cholesteatoma. Laryngoscope. 1994;104(3 pt 2):1-24.
5. Weber PC, Adkins WY Jr. Congenital cholesteatomas in the tympanic membrane. Laryngoscope. 1997;107(9):1181-1184.
6. Nejadkazem M, Totonchi J, Naderpour M, Lenarz M. Intratympanic membrane cholesteatoma after tympanoplasty with the underlay technique. Arch Otolaryngol Head Neck Surg. 2008;134(5):501-502.
7. Grindle CR, Shah GB, O'Reilly RC. Intratympanic membrane cholesteatoma: a rare bilateral presentation within a single-institution case series. Int J Pediatr Otorhinolaryngol. 2011;6(4):373-375.
8. Min HJ, Yoo SW, Lim J, Lee SH. Congenital intratympanic membrane cholesteatoma: report of three cases and review of literature. Korean J Otorhinolaryngol-Head Neck Surg. 2013;56(5):302-305.
9. Lee CH, Kim JY, Kim YJ, Yoo CK, Kim HM, Ahn JC. Transcanal C02 laser-enabled ablation and resection (CLEAR) for intratympanic membrane congenital cholesteatoma. Int J Pediatr Otorhinolaryngol. 2015;79(12):2316-2320.
10. Schwartz RH, Linde RE. Iatrogenic implantation cholesteatoma: an unusual complication of tympanostomy tubes. J Pediatr. 1979;94(3):432-433.
11. Suzuki T, Nin F, Hasegawa T, et al. Congenital cholesteatoma in the tympanic membrane. lnt J Pediatr Otorhinolaryngol. 2007;2(1):48-50.
12. Weber PC, Adkins WY Jr. Congenital cholesteatomas in the tympanic membrane. Laryngoscope. 1997;107(9):1181-1184.
13. Yoshida T, Sone M, Mizuno T, Nakashima T. Intratympanic membrane congenital cholesteatoma. lnt J Pediatr Otorhinolaryngol. 2009;73(7):1003-1005.
14. Pasanisi E, Bacciu A, Vincenti V, Bacciu S. Congenital cholesteatoma of the tympanic membrane. lnt J Pediatr Otorhinolaryngol. 2001;61(2):167-171.
Dr Schwartz is professor of Pediatrics, Virginia Commonwealth University School of Medicine, Inova Children’s Hospital Campus, Falls Church, Virginia. Dr Bahadori is a pediatric otolaryngologist in private practice at Otolaryngology Associates, Fairfax, Virginia. The authors have nothing to disclose in regard to affiliations with or financial interests in any organizations that may have an interest in any part of this article.


11-year-old boy with testicular pain and rash
January 19th 2024An 11-year-old boy presented to the emergency department complaining of left testicular pain for 2 days, described as intermittent and stabbing, which ranged between 5 and 8 of 10 in intensity. Read the full case to see if you can correctly diagnose the patient.

Newborn with midline neck lesion
December 21st 2023A 4-day-old boy with a midline neck lesion was born at term by normal vaginal delivery. After birth, mid line lesion had the configuration of a linear cleft with a cephalocaudal orientation, extending from the level below the hyoid bone to the suprasternal notch with a length of 2.5 cm and a width of 0.5 cm. What's the diagnosis?

A 13-year-old girl with well-demarcated rash on back and chest
October 19th 2023A healthy 13-year-old girl presented with a 1-month history of an asymptomatic, well-demarcated rash on her back and upper chest. The eruption consisted of discrete, dark brown papules that coalesced into large, flat-topped plaques with mild superficial scale and accentuation of skin markings. What's the diagnosis?

Suspicious facial swelling in a 22-month-old girl
October 11th 2023A 22-month-old female patient with sickle cell disease on folic acid and penicillin prophylaxis with a 3-day history of nasal congestion, rhinorrhea, fever and decreased oral intake presents to the emergency department (ED) for acute facial swelling noted when she woke up from a nap. What's the diagnosis?

Friction-induced blistering on a child’s feet
July 14th 2023You are called to the hospital nursery to evaluate a healthy full-term newborn boy who developed painful flaccid blisters and erosions on the tops of his feet and ankles shortly after birth. His mother had a history of similar recurrent skin lesions that healed with scarring. She also had oral and gastrointestinal tract involvement. What's the diagnosis?

