





How to help parents cut healthcare costs
The cost of healthcare can be overwhelming for patients’ families. Here are ways to cut parents’ out-of-pocket medical expenses and even help your bottom line.


These days many families have high-deductible insurance plans, and the cost of healthcare services can be intimidating. Any efforts made by concerned providers to reduce healthcare costs are appreciated by our patient’s families. There is much we can do to keep parents’ out-of-pocket health costs to a minimum.
Some basics
Physicians need to familiarize themselves with patients’ insurance plans. This information is readily available in the patient’s electronic health record (EHR). In general, patients with Medicaid health plans have little responsibility for healthcare expenses. In contrast, parents with either private, employer-provided insurance, or Affordable Care Act (ACA) insurance must pay thousands of dollars toward healthcare expenses until their deductibles are met.
Office visits to pediatricians for non–preventive care visits can total in the hundreds of dollars. This is not to say that are our fees are inappropriate, but many parents postpone visits for ailing children based on cost considerations. This is why we face stiff competition from walk-in clinics that are usually less expensive than physicians’ offices. (See https://www.cvs.com/minuteclinic/services/price-lists for CVS’ MinuteClinic price lists-and compare these to your own.) Although quality care from a familiar provider is considered by most parents a worthwhile investment, some may feel differently when they get your bill.
Discounting services
A medical practice usually adopts 1 fee schedule for all services provided. This is typically a multiple of the published Medicare fees established by the Centers for Medicare and Medicaid Services (CMS). Contracts with insurance companies determine what you get paid for each visit. Whereas a detailed discussion of office fees is beyond this scope of this article, most practices make sure that their fees are higher than the fees allowed by insurance plans to assure optimal payment.
There are, however, several circumstances for which physicians can provide services at reduced fees if circumstances warrant:
· First, a sick visit is charged by most pediatricians as a 99214 or a 99213 visit. This is based on several factors that include the number of problems addressed and medical decision making involved. Physicians do have latitude in charging a visit as a 99213 versus 99214 depending on how the visit is documented.
· Secondly, in many states, physicians can offer discounts for prompt payments. I would recommend checking with your insurance plans as well as your state health insurance department to see if this is allowed. If so, parents appreciate a reduction (20% to 30% is reasonable) in their bill, and prompt payment improves your office cash flow.
· Lastly, in most states, noninsured patients can be charged at a reduced rate. Again, check your insurance plans and the state health insurance department to check state regulations, but discounting a charge by up to 30% makes sense for the uninsured and makes seeking healthcare services from a primary care physician less foreboding.
In addition, because well visits are typically covered in their entirety by health insurance plans, minor problems can be addressed at these visits. If we discover an ear infection, for example, we can theoretically bill for a separate ill visit encounter-or not-depending on the amount of “extra” effort involved. Some physicians refill meds for attention-deficit/hyperactivity disorder (ADHD) at a yearly physical at no extra charge to the patient.
Best prices for services
Whereas the above can be controlled by providers, there are many external healthcare expenses beyond physician control. Services such as lab tests and x-rays are performed by local labs, imaging centers, or local hospitals, and these costs add up quickly. It is up to pediatricians to decide whether such tests are necessary.
Recommended: 2017's best tech for the pediatrician
Often experienced pediatricians can diagnose many conditions based on history and physical examination alone. We often don’t need x-ray confirmation of a suspected pneumonia. We don’t need a positive respiratory syncytial virus (RSV) test or complete blood count (CBC) to diagnose bronchiolitis. Each situation is different but, as we all know, we need to be careful and cautious depending on the age of the patient, the symptoms, and whether the result of a particular test makes a difference in the care being rendered. Liability factors into this decision as well. Patients with injuries often need an x-ray to rule out significant or subtle fractures. Patients with a history of prolonged or worsening headaches may eventually require a magnetic resonance imaging (MRI) study to rule out a brain tumor.
NEXT: Cost comparisons of an MRI


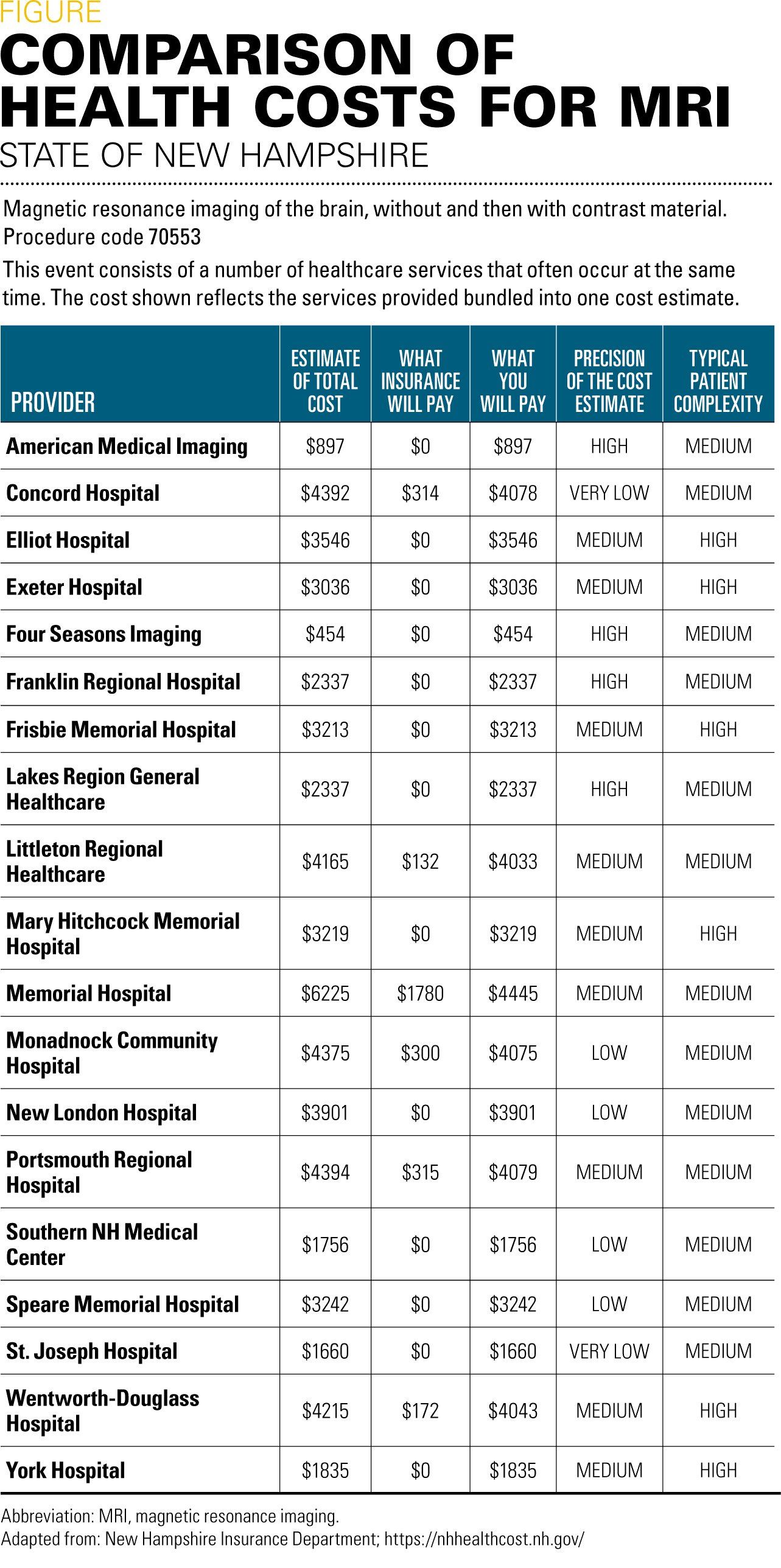
We need to realize that prices for services vary significantly from one facility to another. Many states have websites where average charges for medical services are posted, based on the procedure, the insurance plan, and the facility performing the service. I practice in New Hampshire, and according to the nhhealthcost.nh.gov website established by the New Hampshire State Insurance Department (Figure), one hospital in the state charges noninsured patients $800 for a computed tomography (CT) scan while another charges $3200 for this service. If you have Harvard Pilgrim insurance in New Hampshire, a brain MRI will cost as little as $454 or as much as $4400. Similarly, a CBC in New Hampshire for an uninsured patient will cost from a low of $15 to a high of $105 dollars, while for an insured patient the out-of-pocket cost would be $11 to $89. It would be worth your while to do some research and investigate the most cost-effective services for your patients, taking quality, reliability, and location of the service into account as well.
NEXT: Reducing pharmacy costs
Reducing pharmacy costs
Another way to save our patients’ money is to be cognizant of the cost of the medications we prescribe. Competition is fierce among pharmacies and even medication that we assume is inexpensive varies in price from one pharmacy to another. Amoxil is probably the least expensive medication we prescribe. The 400-mg suspension bid for 10 days in my area costs $4 at Walmart and $11 at CVS-not all that much different. In contrast, a month of 20-mg generic Adderall XR will cost noninsured patients $167 at Walmart and $67 at Walgreens. It is prudent to familiarize yourself with several insurance plan formularies so you can prescribe the lowest-priced but most-effective medication.
Mobile apps that save patients money
One of my top 10 apps for pediatric practice is GoodRx, available as a mobile application or web portal. I have saved patients hundreds of dollars by recommending this application because it displays coupons that reduce the cost of prescriptions, sometimes below that of insurance copayments. The app is free and worth recommending to your patients’ parents.
Another app worth recommending to parents that can prevent unnecessary expenditures is the $2.99 SymptomMD. It is an application all parents should use to self-triage medical problems. It includes dosages of commonly used medications such as acetaminophen, diphenhydramine, and ibuprofen, and provides sage advice regarding what symptoms warrant observation, prompt evaluation by a physician, or an emergency department (ED) visit. As discussed in my previous article (“Top 10 apps for pediatrics,” Contemporary Pediatrics, February 2017), the application has been shown to reduce unnecessary visits to physicians and EDs.
Change your practice!
Those pediatricians who are young and adventurous, or mature pediatricians who are frustrated with the status quo, should consider changing their practice model. You can practice a more cost-effective type of medical practice that increases the time spent with patients while reducing patient costs by converting your practice to direct primary care. This is a practice model that is subscriber based. Patients pay a fixed monthly fee, typically of the magnitude of $60 to $70 per month per enrolled patient. Patients are seen for unlimited well and sick visits without a copay, with office tests provided at no charge. Patient still maintain insurance for hospitalizations and ED visits.
Next: How to avoid missteps when prescribing medications
The benefit is that pediatricians can usually cap their patient panel at less than 1000 patients, compared with the 2000 or more patients that is typical for those accepting standard insurance. Your office overhead is reduced because you no longer need to bill insurance or process claims. Pediatricians with reasonable overhead can earn more than they could in a standard practice, yet the price to the parent is dramatically less than it would be otherwise. This is why direct primary care is growing rapidly.
In conclusion
The cost of healthcare can be overwhelming for many of our patients’ families, and the suggestions I have given can significantly reduce parents’ out-of-pocket medical expenses. Please contact me at medgizmos.com if you’ve discovered any other ways to reduce medical costs for your patients!











Anger hurts your team’s performance and health, and yours too
October 25th 2024Anger in health care affects both patients and professionals with rising violence and negative health outcomes, but understanding its triggers and applying de-escalation techniques can help manage this pervasive issue.




