





Hypothermia and emesis in a newborn
The patient, a 7-day-old, small-for-gestational-age female (birth weight, 2.21 kg), born by vaginal delivery at 37 weeks to a G1P0 mother, presented to the pediatric emergency department for hypothermia and emesis at the recommendation of her pediatrician.





The Case
The patient, a 7-day-old, small-for-gestational-age (SGA) female (birth weight, 2.21 kg), born by vaginal delivery at 37 weeks to a G1P0 mother, presented to the pediatric emergency department (ED) for hypothermia and emesis at the recommendation of her pediatrician. The neonate's delivery was complicated by maternal and newborn fever, and she received antibiotics for 48 hours. Ultimately, her blood cultures were negative. Otherwise, she did well in the nursery and was discharged at 2 days of age.
After discharge, the baby was breastfeeding without emesis, and although she was thought to be sleepy (by mother's report), she did wake for feeds. At baseline, she breastfed for 5 to 10 minutes every 3 to 4 hours, but starting at age 5 days she was having greater difficulty latching. Furthermore, she became lethargic and developed nonbilious, nonbloody, nonprojectile emesis with each feed.
The neonate maintained continued daily bowel movements. Simultaneously, she had decreased urine output, with 2 small wet diapers the night prior to admission. The morning of admission, the patient was taken to her pediatrician, who noted a rectal temperature of lower than 36°C, along with emesis with feeding trial.
NEXT: What's the diagnosis?
Physical exam
In the pediatric ED, the patient weighed 2.20 kg and had a rectal temperature of 35.8°C, heart rate of 138 beats per minute, respiratory rate of 32 breaths per minute, and a blood pressure of 77/51 mm Hg. Physical exam revealed an active and alert neonate in no apparent distress; her abdomen was soft, nontender, nondistended, and without hepatosplenomegaly. The remainder of the examination was noncontributory.
Differential diagnosis
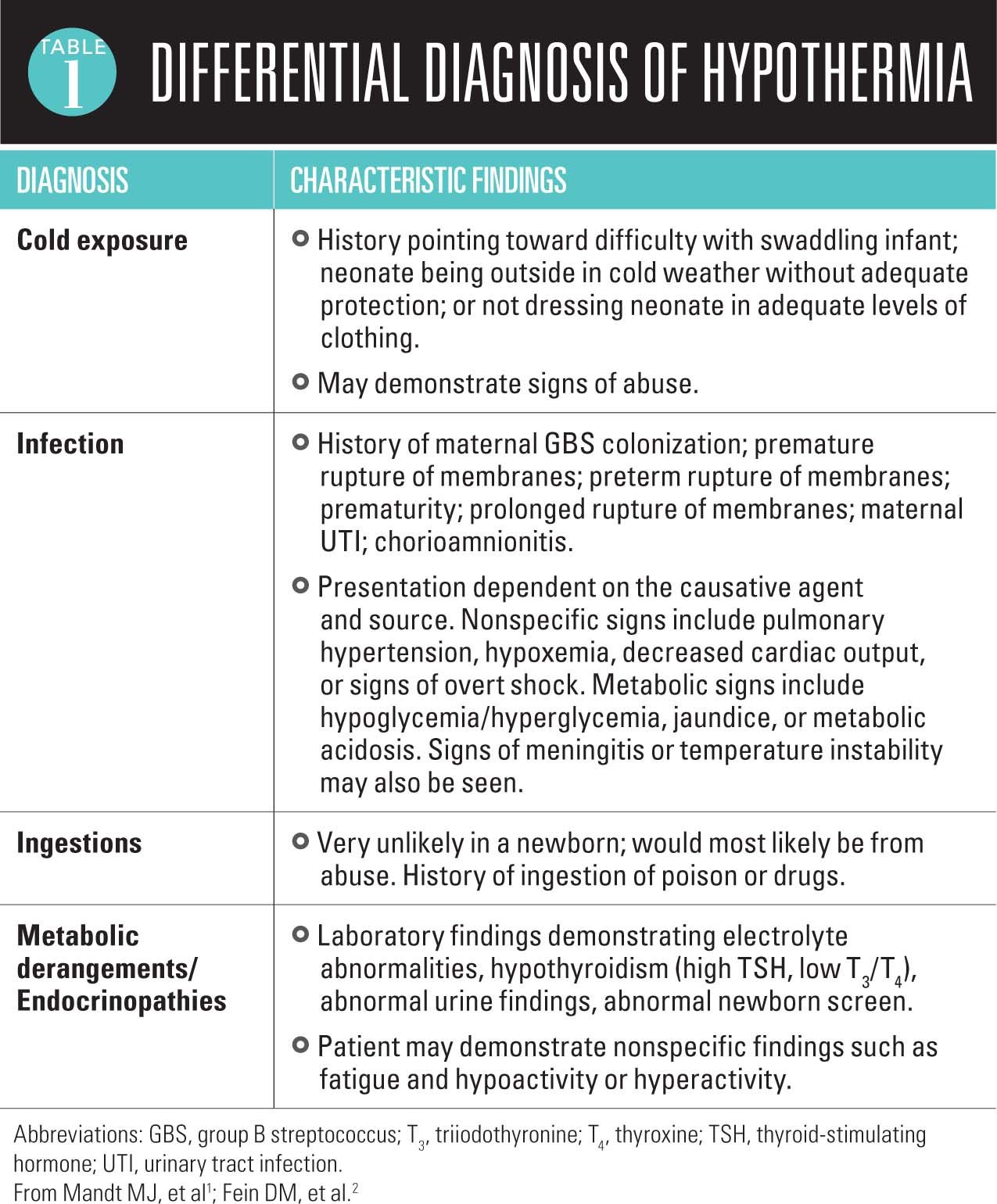
The patient presented with 2 primary symptoms, both of which have unique differential diagnoses. Hypothermia in a newborn is concerning for many possible conditions (Table 11,2). Although the definition is controversial, the World Health Organization (in 1997) categorized hypothermia as an unintentional temperature drop below 36.5°C and further divides hypothermia into 3 stages: cold stress (36.0°C-36.4°C), moderate hypothermia (32.0°C-35.9°C), and severe hypothermia (<32.0°C).3 Neonates are at higher risk of developing hypothermia because of their large surface-to-mass ratio, lack of subcutaneous tissue, and poorly developed thermoregulation. Hypothermia may occur secondary to environmental exposure, infections (sepsis, meningitis), metabolic/endocrine disorders, drugs, central nervous system dysfunction, shock, burns, or iatrogenic causes.2


More: Boosting micropreemie outcomes
The initial concern in this neonate with hypothermia was a serious bacterial infection, which should be considered highly until proven otherwise. The patient's concurrent lethargy and emesis in the context of peripartum maternal fever could have been consistent with an undertreated infection or late-onset infection. Although lower on the differential, metabolic derangement was considered given the patient's emesis, which would lead to electrolyte imbalance and nutritional deficiency, ultimately resulting in hypothermia. The lack of history of cold exposure and ingestions made these diagnoses less likely in this neonate.
NEXT: Differential diagnosis of emesis


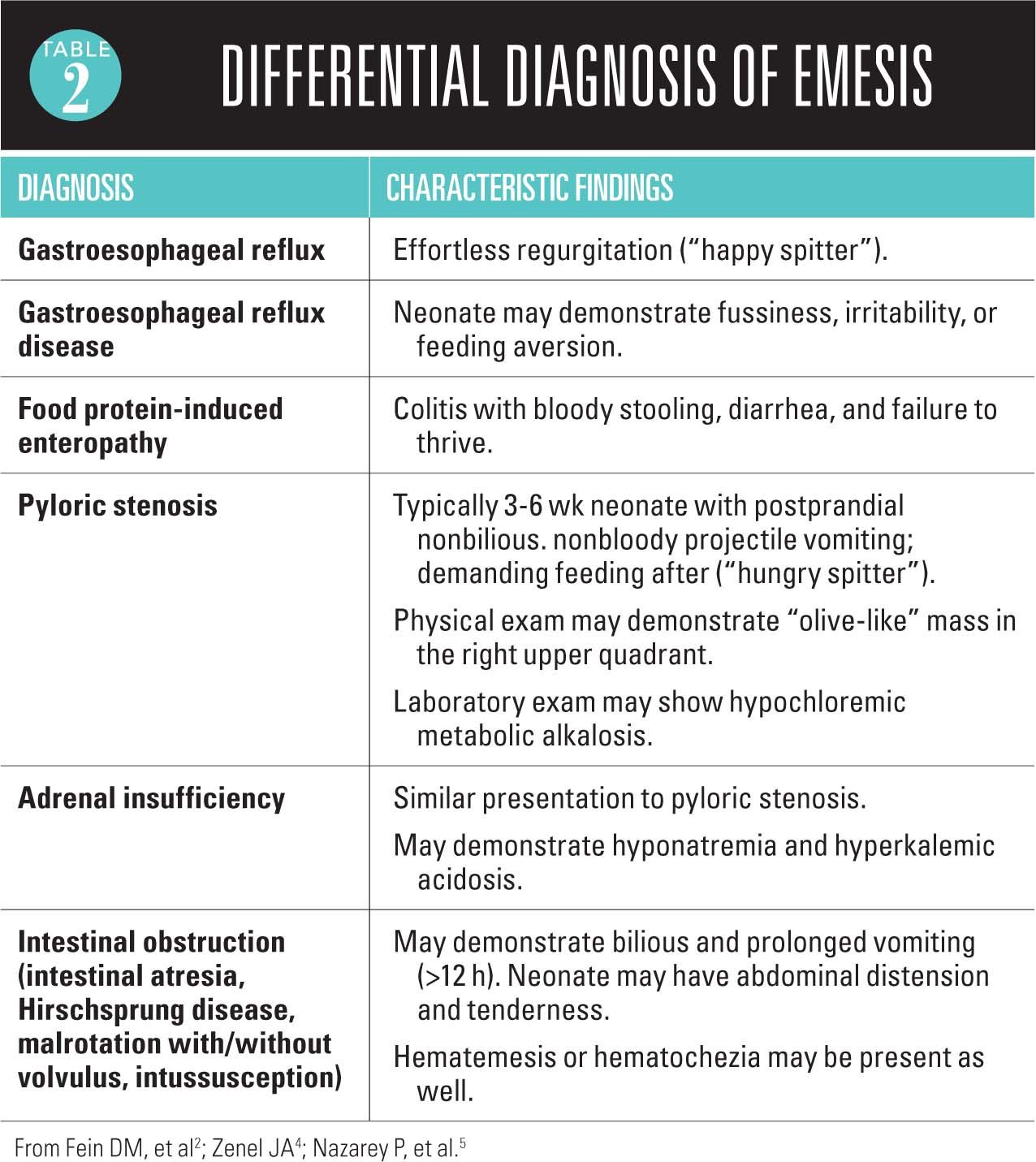
Emesis in the newborn also can be attributed to a myriad of pathologies. Primary diagnoses include gastroesophageal reflux/gastroesophageal reflux disease, feeding intolerance, obstruction, necrotizing enterocolitis, metabolic disorders, milk-protein intolerance, and infections (urinary tract infection or meningitis; Table 22,4,5).6 Given the hypothermia and history of peripartum maternal fever, infection was the top diagnosis in the differential. Suspicion for a primary gastrointestinal etiology was initially lower on the differential because the newborn presented with normal stooling and intermittent spit-up.
Laboratory tests
Workup for infectious etiology revealed normal urinalysis, complete blood count, and comprehensive metabolic panel. A respiratory viral panel was negative, and a bloody lumbar puncture was significant for elevated protein (839 mg/dL). At 48 hours into the evaluation, all cultures and the herpes simplex virus polymerase chain reaction test were negative. Antibiotics were discontinued but emesis persisted. During the first 24 hours in the hospital, the patient had 6 episodes of nonbilious, nonbloody emesis described as "spit-up." She was started on ranitidine with little relief.
Recommended: Toddler with blistering acrodermal rash
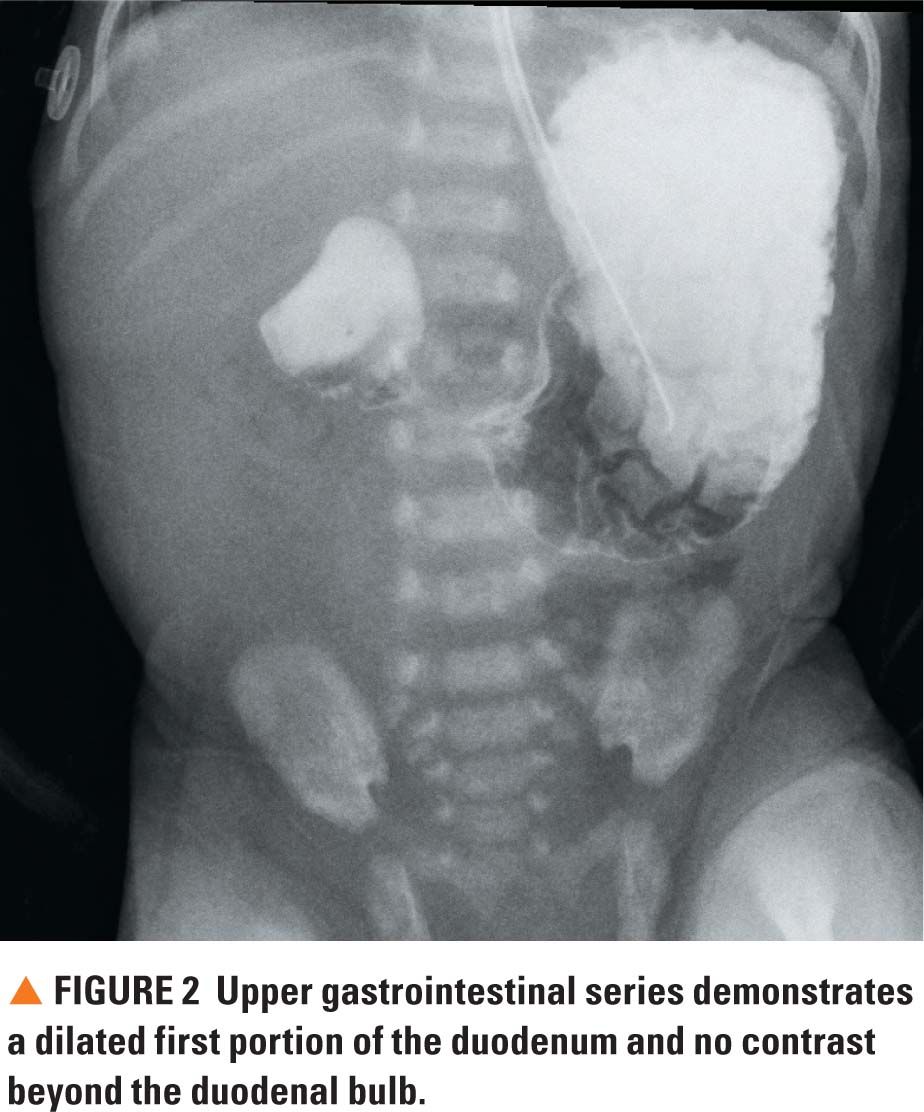
Throughout the hospital course, emesis occurred either immediately after feeds or within 30 minutes, varying in quantity between 10 mL and 40 mL. The patient continued to have bowel movements and a benign abdominal exam. However, given the emesis, nasoduodenal (ND) tube placement was attempted on day 2 of the admission. This procedure was unsuccessful and an abdominal X-ray at the time of placement demonstrated the ND tube tip within the region of the stomach along with gaseous distension of the stomach and an enlarged duodenal bulb (double bubble; Figure 1). The X-ray also showed minimal distal gas in the bowel in the left lower quadrant and an overall paucity of bowel gas. While awaiting further imaging in the radiology suite, the patient had her first episode of bilious vomiting. Upper gastrointestinal (GI) series demonstrated dilatation of the first portion of the duodenum without contrast beyond the duodenal bulb (Figure 2).
Given these findings, intestinal obstruction became the leading diagnosis, although the patient's hypothermia could have been explained by being SGA at birth (with resultant impaired thermoregulation), or by infection.4,5
NEXT: Diagnosis and discussion
Diagnosis
Pediatric surgery was consulted. The patient underwent an exploratory laparotomy that revealed an annular pancreas with duodenal stenosis above the level of the common bile duct, as well as malrotation. No ischemic bowel changes were noted.
Discussion
Overall, congenital duodenal obstruction affects 1 in 2500 to 1 in 10,000 live births.7 In 1980, Kiernan and colleagues published a seminal review of annular pancreas, which encompassed 266 literature reports and 15 operations at the Mayo Clinic between 1957 and 1976.8 In this series, 51.5% of cases of annular pancreas occurred in children, and almost all neonates presented unable to swallow secretions or by vomiting feedings, usually with first feed.4,5,8 This finding is supported by a review by Chen and associates from records at the Children's Hospital of Zhejiang University School of Medicine, China.7 Among the 287 neonates identified in their facility with duodenal obstruction, 86.06% of patients presented with vomiting and 83.81% with bilious vomiting.
Next: Toddler with spiking fevers and persistent rash
However, the patient in this case had an atypical presentation, with hypothermia occurring later in the first week of life and nonbilious vomiting that appeared more characteristic of "spit-up." Interestingly, the patient developed bilious vomiting while in the radiology suite. Because the lesion was above the level of the common bile duct, likely there was an accumulation of bile that led to the more traditionally seen emesis pattern.9,10


Clinical presentation of different medical conditions often can be subtle in newborns. The presentation of gastrointestinal obstruction is clear when a patient presents with early projectile and/or bilious vomiting combined with absent flatus or bowel movements. However, as in this case, the clinical picture can be obscured when a neonate presents with nonbilious emesis, and complicated further by hypothermia and lethargy, which suggest an infectious etiology until proven otherwise.
This case underscores the importance of having a high index of suspicion for neonatal bowel obstruction, particularly in babies presenting with vomiting (regardless of the character or timing) and systemic signs of illness. Additionally, pediatricians should have a low threshold for ordering abdominal imaging in neonates presenting with emesis. If an abdominal X-ray demonstrates a pattern of general gas paucity, clinicians should perform additional radiographic imaging (such as an upper GI series or abdominal sonogram) to evaluate for a possible bowel obstruction.
Patient outcome
The patient underwent an uncomplicated duodenoduodenostomy and was safely discharged 20 days after the surgery.
REFERENCES
1. Mandt MJ, Grubenhoff JA. Emergencies and injuries. In: Hay WW Jr, Levin MJ, Deterding RR, Abzug MJ, Sondheimer JM. Current Diagnosis and Treatment: Pediatrics. 21st ed. New York, NY: McGraw-Hill Companies; 2012:351-352.
2. Fein DM, Avner JR. The febrile or septic-appearing neonate. In: Schafermeyer RW, Tenenbein M, Macias CG, Sharleff GQ, Yamamoto LG. Strange and Schafermeyerâs Pediatric Emergency Medicine. 4th ed. New York, NY: McGraw-Hill Education; 2015:5-7.
3. Kumar V, Shearer JC, Kumar A, Darmstadt GL. Neonatal hypothermia in low resource settings: a review. J Perinatol. 2009;29(6):401-412.
4. Zenel JA. Examination of the newborn infant. In: Rudolph CD, Rudolph AM, Lister GE, First LR, Gershon AA. Rudolphâs Pediatrics. 22nd ed. New York, NY: McGraw-Hill Companies; 2011:174-183.
5. Nazarey P, Sato TT. Gastrointestinal obstruction. In: Rudolph CD, Rudolph AM, Lister GE, First LR, Gershon AA. Rudolphâs Pediatrics. 22nd ed. New York, NY: McGraw-Hill Companies; 2011:1394-1395.
6. Parashette KR, Croffie J. Vomiting. Pediatr Rev. 2013;34(7):307-319.
7. Chen QJ, Gao ZG, Tou JF, et al. Congenital duodenal obstruction in neonates: a decadeâs experience from one center. World J Pediatr. 2014;10(3):238-244.
8. Kiernan PD, ReMine SG, Kiernan PC, ReMine WH. Annular pancreas: Mayo Clinic experience from 1957 to 1976 with review of the literature. Arch Surg. 1980;115(1):46-50.
9. Merianos DJ, Schwab CW II. Pediatric surgery. In: Atluri P, Karakousis GC, Porrett PM, Kaiser LR. The Surgical Review: An Integrated Basic and Clinical Science Study Guide. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:382-393.
10. Hackam DJ, Grikscheit T, Wang K, Upperman JS, Ford HR. Pediatric surgery. In: Brunicardi FC, Anderson DK, Billiar TR, et al. Schwartz's Principles of Surgery. 10th ed. New York, NY: McGraw-Hill Companies; 2014;chap 39.
Mr Wei is a fourth-year medical student at Weill Cornell Medicine, New York-Presbyterian Hospital, New York City, New York. Dr Spigland is professor of Clinical Surgery, Weill Cornell Medicine, and chief, Division of Pediatric Surgery and Pediatric Trauma, New York-Presbyterian Hospital, Cornell Campus. Dr Green is assistant professor of Pediatrics, Weill Cornell Medicine, New York-Presbyterian Hospital, New York City. The authors have nothing to disclose in regard to affiliations with or financial interests in any organizations that may have an interest in any part of this article.

















