





Common pediatric allergy-related disorders
An overview of disorders related to allergic symptoms in the pediatric patient, such as rhinitis, otitis media, asthma, and atopic dermatitis, as well as guidence regarding when to refer to an allergist.


Rhinitis
Rhinitis, or inflammation of the nasal mucosa, most often presents with rhinorrhea, congestion, sneezing, and sometimes itching of the nose, throat, eyes, or ear canals. Rhinitis may be nonallergic, allergic, or both. Nonallergic causes may be more common in the child younger than 2 years, and most often is infectious rhinitis, which usually is viral. Nonallergic causes in the older child may include vasomotor or idiopathic nonallergic rhinitis. Allergic rhinitis is generally classified as seasonal or perennial allergic rhinitis, based on the pattern of symptoms throughout the calendar year.
How to treat rhinitis
Many pediatricians and primary care providers treat patients with rhinitis presumptively for allergy by prescribing antihistamines, decongestants, or intranasal steroid sprays. Empiric treatment is a reasonable first approach. It also may provide the physician with additional information, especially if the medication dose is appropriate, and is used judiciously in the proper population. A positive response to antihistamine therapy is generally regarded as indicating that the patient's symptoms are mediated by histamine release, signaling underlying allergic disease. However, if treatment includes a first-generation antihistamine (available over the counter), the anticholinergic properties of the antihistamine may be responsible for mucosal drying. This is an apparently positive response seen in both allergic and nonallergic disease.
When to refer the child with rhinitis


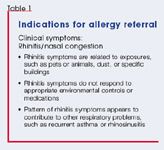
One factor that may strengthen the indication for referral is the manifestation of symptoms of food allergy. Studies show that food allergy is usually the first specific IgE response that an atopic child develops-often in infancy. Although food allergy may produce rhinitis symptoms, they almost always arise in association with other allergic manifestations, such as a rash or gastrointestinal symptoms.2 The development of food allergy in infancy is highly predictive of the development of inhalant sensitivity later in childhood.3,4
Through high-level exposure, a child younger than 2 years may develop an allergic response to a ubiquitous allergen such as a house dust mite or animal dander in the home. But development of significant allergic symptoms to an inhalant allergen that is present during a single season of the year is unusual in a child of this age.5 The decision to refer a young child for allergy testing/evaluation is also complicated by the frequency of viral upper respiratory infections in children of this age. But because parents often are unable to distinguish symptoms of viral infection from those of allergy, referral may be as valuable for ruling out allergy in this age group as it is for confirming it.










Recognize & Refer: Hemangiomas in pediatrics
July 17th 2019Contemporary Pediatrics sits down exclusively with Sheila Fallon Friedlander, MD, a professor dermatology and pediatrics, to discuss the one key condition for which she believes community pediatricians should be especially aware-hemangiomas.





