The essentials of pediatric ECGs, Part 1
Interpreting pediatric ECGs



Keypoints:
Waves, squares, tracings, line segments, grids...all set against salmon-colored paper! It can be frustrating to deal with, but you can decipher pediatric ECGs without breaking a sweat.
Although pediatric patients do not routinely have electrocardiograms (ECGs), there are times for their inclusion. Symptoms of chest pain, syncope, or palpitations, first degree relatives with significant dysrhythmia or cardiomyopathy concerns, or the initiation of rhythm-altering behavioral medications are all suitable instances for the use of a pediatric ECG. But as many practitioners have learned first-hand, interpreting the data from this roll of paper can be anything but straightforward-occasionally stirring up copious amounts of aggravation. A firm understanding of the fundamental principles of ECG can quell this reaction, and help guide your clinical decisions.
In general, you should analyze a pediatric ECG (or one for any age range) with respect to the following eight parameters:
Part 1 of this article examines the first four principles required for basic ECG interpretation. The remaining parameters will be discussed in the October 2007 issue of Contemporary Pediatrics.
1 General quality/technique
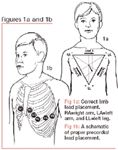
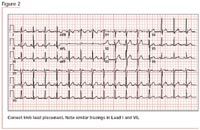
Accurate assessment of an ECG naturally requires proper test set-up. With that, the ECG should have a minimum of 12 leads: six limb leads (Leads I, II, III, aVR, aVL and aVF) and six precordial leads (V1 to V6).