





Juiced: What kids do to compete
Pediatric sports and activity participation is on the rise. It is estimated that up to 45 million children are involved in some form of athletics.1 On the whole, exercise is something to be encouraged in today’s children, with benefits of improving physical fitness, increasing social interaction with peers, decreasing stress, achieving self-efficacy, and gaining experience in goal setting, teamwork, and commitment.
Pediatric sports and activity participation is on the rise. It is estimated that up to 45 million children are involved in some form of athletics.1 On the whole, exercise is something to be encouraged in today’s children, with benefits of improving physical fitness, increasing social interaction with peers, decreasing stress, achieving self-efficacy, and gaining experience in goal setting, teamwork, and commitment.
More: Mouth guard do's and don't's
With the increase in the number of children involved in sports, however, there is also an increase in competition. Athletes and their families look for ways to rise above their competitors and gain an advantage. It is now common for young athletes to specialize in a single sport early on and play year round. Today’s children work with personal trainers, strength coaches, nutritionists, and skill specialists. The “off–season” has become obsolete for many young athletes. Parents are investing significant time and money into helping their children gain a competitive edge because often that edge increases the likelihood of success. How kids train, where they train, who they work with, and what they use are all factors in today’s sports culture.


Sports nutrition is an influential tool in the athlete’s toolbox. Adjustments in nutritional status can be done safely to improve energy balance, reduce fatigue, support bone and muscle growth, increase bone mass, and aid in muscle contraction. Societal and individual pressures to “be the best” and “win at all costs,” however, push an increasing number of athletes to experiment with performance-enhancing substances (PES), including supplements, energy drinks, prescription medications, and banned/illicit substances.2
Sports nutrition
Like choosing the fuel for a car, the food that an athlete consumes directly affects performance. Athletes strive to be at their best and, along with their parents, seek guidance on ways to be stronger, leaner, and able to withstand the demands of training and competition. As medical providers, this is an opportunity not only to screen for nutritional issues and PES use but also to educate regarding nutritional needs in growing, active bodies.
Diets with insufficient nutrients provide suboptimal fuel for workouts, increase the risk of nutrient deficiencies that can lead to illness or fatigue, and can hinder bone and muscle growth and recovery. Sports nutrition focuses on proper intake of macronutrients (carbohydrates, protein, fat) and micronutrients (calcium, iron, folate, vitamin B6, zinc).3 Research shows that insufficiencies exist in adolescent diets, particularly in athletes participating in sports with an emphasis on body composition and appearance (wrestling, gymnastics, dance).4 An overview of critical micronutrients is provided in Table 1.1,2
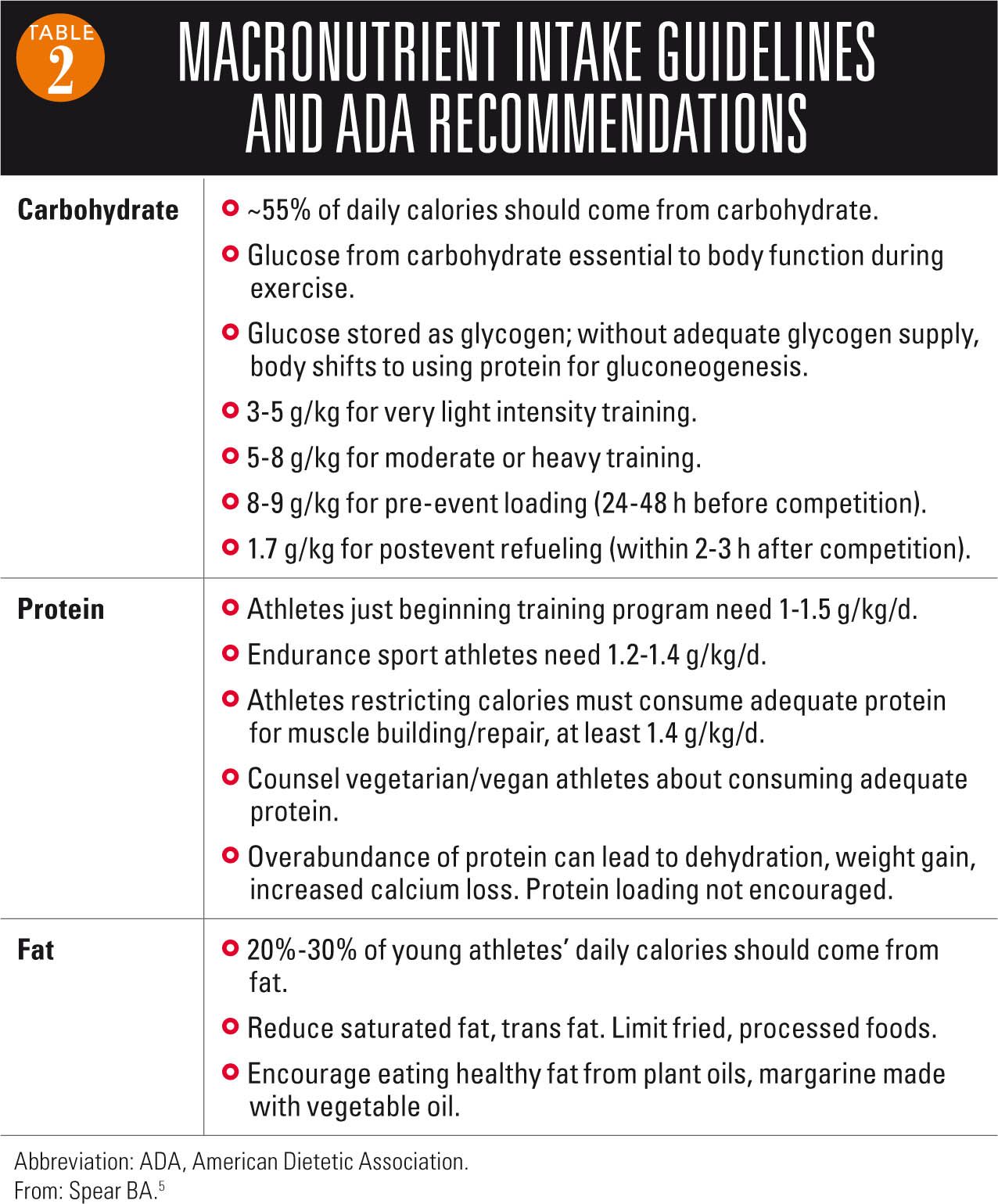
Proper intake of macronutrients is essential for energy balance. Carbohydrates are the main fuel during athletic activity. Protein is critical to muscle building, maintenance, and repair. Fat is a major energy source, particularly during light-to-moderate intensity exercise and endurance sports. Restriction of fat and increased consumption of protein are increasingly common practices in the young athletic population.2 These can be healthy modifications when done within reason, but should still be part of a well-balanced diet and not taken to the extreme. Recommendations regarding macronutrient intake are summarized in Table 2.5
NEXT: Making the most of anticipatory guidance


Hydration
Keeping athletes well hydrated during activity is important for maintaining performance and regulating body temperature. Hydration before, during, and after activity should be part of each athlete’s routine. Children and adolescents are at higher risk of dehydration compared with adults because of a higher body surface area to body mass ratio, decreased efficiency at transporting heat to the skin, and increased heat production during exercise.6
Recommended: Are kids eating too much pizza?
All beverages provide hydration, but research consistently shows that water is the drink of choice for sports lasting less than 1 hour of exertion.7 For these shorter events, replacing water (rather than glucose, electrolytes) is the main concern. For children doing prolonged or vigorous intensity exercise lasting longer than 60 minutes, loss of water and electrolytes will increase. Studies have shown that consuming a sports drink containing carbohydrates in these instances helps avert fatigue and maintain performance.
Caution should be exercised, however, when selecting a rehydration drink. In the majority of young athletes, water is appropriate and should be encouraged as the first choice. For the average child doing routine activity, sports drinks are not necessary and expose kids to added sugar and calories without significant nutritional value. Sports drinks contain 2 g to 19 g of carbohydrate per serving and range from 10 to 75 calories per serving.8,9 They are not indicated for use during meals or snacks, and sports drinks should not be a regular substitute for water or low-fat milk.9
Advocacy and action is needed because advertisements aimed at young people blur the impression of what is healthy, and daily access to unhealthy choices continues. Although full-calorie sodas are being removed from school vending machines, beverage manufacturers are replacing them with sports drinks. In 2006, sports drinks were the third fastest-growing beverage category in the United States after energy drinks and bottled water. The trade group representing beverage manufacturers reported that sports drinks increased their market share in schools from 14.6% in 2004 to 20% during the 2006–2007 school year.8
NEXT: Sports drinks versus energy drinks
Sports drinks vs energy drinks
Although the terms are often used interchangeably, it is important to note that sports drinks and energy drinks are not the same. The main ingredients and the intended uses are very different, yet often this is not realized by the young athletes who consume them or by the parents who provide them. Sports drinks are beverages designed to replenish water and electrolytes lost during exercise. They may contain carbohydrates, minerals, electrolytes, and flavoring. In contrast, energy drinks are beverages advertised to boost energy, decrease fatigue, improve concentration, and increase mental alertness. These effects are attributed to the inclusion of nonnutritive stimulants, including caffeine, guarana, taurine, ginseng, L-carnitine, creatine, and glucuronolactone.9


The actual amount of stimulant in many energy drinks is not specified on the container or able to be found on the Internet, and the majority of energy drinks contain multiple stimulants, which increases concern for adverse effects. For example, caffeine and guarana are often used together in energy drinks. Yet, guarana is a plant extract that contains caffeine; 1 g is equal to approximately 40 mg of caffeine.9 The total amount of caffeine contained in some products exceeds 500 mg (equivalent to 14 cans of common caffeinated soft drinks).
Recommended: When pill parties turn deadly for teens
Protein and amino acids are also advertised in sports and energy drinks, often purported as “muscle recovery” drinks. Clinical trials have not supported their use in young athletes. Research has not shown an advantage in consuming these drinks over healthy food choices. In fact, low-fat chocolate milk is just as good, if not better, an option for postexercise protein recovery. The American Academy of Pediatrics (AAP) discourages use of energy drinks or stimulant-containing beverages in children and adolescents.1,7


NEXT: What's the definition of PES?
PES: definition and legislation
The AAP defines a PES as “a substance taken in nonpharmacologic doses specifically for the purposes of improving sports performance. A substance should be considered performance enhancing if it benefits sports performance by increasing strength, power, speed, or endurance (ergogenic) or by altering body weight or body composition. Furthermore, substances that improve performance by causing changes in behavior, arousal level, and/or perception of pain should be considered performance enhancing.”10
More: Care of the student athlete
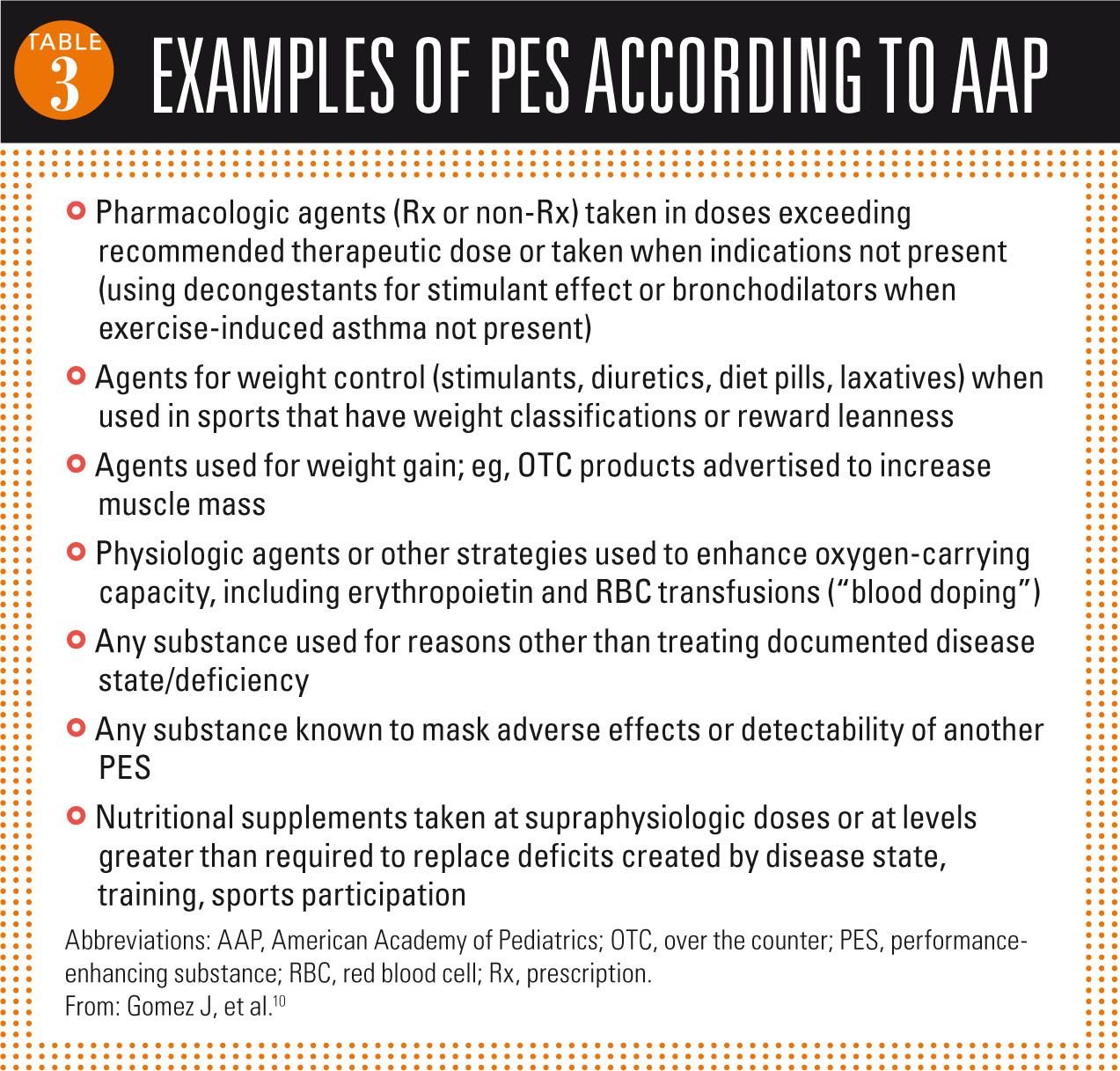
A considerable amount of research has been done on these substances in the last few decades. However, data are lacking on the effects in children and adolescents. Despite the lack of reliable clinical data, these substances continue to be used by athletes to boost performance and by nonathletes to improve appearance and self-image. Examples of PES are listed in Table 3.10
The use of products to improve athletic performance is nothing new. There is evidence that Olympians used mushrooms, strychnine, and dried figs to increase strength, focus, and endurance as early as 776 BC.11 Drug testing and legal consequences are intended to deter use of PES, but the focus has been on collegiate and professional athletes.12 There has been relatively little effect on high school and youth athletes.


A 1995 US Supreme Court ruling authorized school drug testing for student athletes, however, the National Federation of State High School Associations reported only 13% of high schools actually test their student athletes.13 The majority of these schools focus drug testing on marijuana, opiates, and alcohol. Less than a third include steroids or substances common in the athletic/gym culture.11
Societal, personal pressures
Performance-enhancing substances are used widely among children and adolescents. Children are exposed to these substances at younger ages than in years past because of increased marketing and anecdotal evidence in the sports community. Elementary and middle school athletes are being taken to travel team practices long distances from home, and many are working with personal trainers and specialized coaches. Professional scouts now follow high school athletes, and collegiate coaches can be seen scoping out youth tournaments.
The cost of education is also on the rise, and for many families, athletics is the ticket to higher education. There are pressures to excel in academics, in athletics, and in the social scene. These pressures are falling on younger, more impressionable shoulders than ever before. Children and adolescents turn to PES to gain a competitive edge or an emotional boost. Athletes seek to improve performance. Nonathletes may see PES as a way to increase social acceptance, step up their school performance, or improve physical appearance. The potential for serious health complications is overshadowed by the potential for success, status, and respect.
NEXT: Supplements
Supplements
A dietary supplement is defined as “a product (other than tobacco) that is intended to supplement the diet. It bears or contains 1 or more of the following dietary ingredients: a vitamin; a mineral; an herb or other botanical; an amino acid; a dietary substance to supplement the diet by increasing the total daily intake; or a concentrate, a metabolite, constituent, extract, or combination of these ingredients.”10 It is intended for ingestion in the form of a pill, capsule, tablet, or liquid. Dietary supplements also are not recommended “for use as a conventional food or as the sole item of a meal or diet.”10 There is a lack of regulation on safety and distribution because approval by the US Food and Drug Administration (FDA) is not necessary for these products to reach the marketplace.14 Manufacturers’ claims do not need to be proven before appearing on labels. The burden of proof is on the FDA.
More: Insufficient evidence for iron screening in kids
Children and adolescents have easy access to supplements in health food stores, local supermarkets, and large chain retailers. A wide array of powders, drinks, pills, and bars are available to customers with claims of increasing muscle, decreasing fat, gaining weight, shedding pounds, increasing focus, improving endurance, reducing hunger, and boosting energy. It’s a proverbial candy store for athletes. Creatine is one of the most commonly used supplements by young athletes. Other substances used for the goals of enhancing performance include vitamins B and E, chromium, vanadium, L-carnitine, and sodium bicarbonate.12
Creatine is a common supplement used by young athletes and is easily found over the counter (OTC). Research shows that 8.2% of high school athletes use creatine, with up to a third of those students reporting daily use.12 National use by all adolescents is certainly more, given that these studies have looked only into use by athletes.
Creatine is a substance found naturally in the body, particularly in skeletal muscle. It is commonly used by athletes to increase how quickly energy is supplied to muscle by helping generate adenosine triphosphate (ATP). It increases protein synthesis and water retention, allowing muscle cells to become bigger and heavier. Athletes supplementing with creatine have been found to break down less protein in the body and show more muscle strength earlier in training sessions.12 The greatest benefit seems to be in short-burst, repetitive actions such as wrestling and weightlifting. It is commonly taken before and after workouts.
The most common adverse effects of creatine are muscle cramping and intestinal discomfort. Insufficient research has been done on the effects in young athletes, and the bulk of studies have tested the manufacturer’s “recommended” doses of 5 g/day rather than the commonly used doses of 20 to 30 g/day among athletes.12 The American College of Sports Medicine (ACSM) recommends creatine not be used by anyone aged younger than 18 years.11 Collegiate teams are prohibited from supplying creatine or other supplements directly to their student athletes.


Prescription drug use
Prescription medication use is also prevalent in sports.15 Beta agonists are used for stimulation in competition, however, nonathletes have used them to add definition to muscle (by stimulating fat breakdown). They are banned by the International Olympic Committee if there is no medical indication. Interestingly, the percentage of Olympic athletes with a documented diagnosis of exercise-induced asthma increased from 15% in 1984 to 60% in the 1996 Olympic games.12 Beta blockers are used in accuracy sports to control anxiety. Diuretics are used to shed weight quickly and define muscle mass, effects commonly appealing to wrestlers. Narcotics help to decrease pain and consequently allow continued participation.
NEXT: What about banned substances?
Banned substances
There is an extensive list of substances banned by the major governing bodies in sports, and although some of these substances may seem unlikely to show up in our local schools (human growth hormone [HGH], antiestrogens, erythropoietin), several including stimulants and caffeine are commonplace in the United States today. Anabolic steroids are the most common banned substance found on positive drug tests in competitive athletes.12 Used predominantly by male athletes, anabolic steroids are also being used by female athletes and nonathletes. Studies show estimates of anabolic steroid use of 4% to 11% in high school boys and up to 3.3% in high school girls.11 The Centers for Disease Control and Prevention (CDC) found that 6.4% of 12th grade boys had tried steroids; nearly a third of these students were nonathletes.16
Recommended: Treating injuries in the wilderness
Anabolic steroids are used to increase muscle strength and size, increase body weight, and decrease the effects of cortisol to essentially preserve muscle mass. Although the emotional effects of steroids are often discussed as an adverse effect, research is now showing the increased aggression as an attraction for young athletes. Adolescent males have admitted that the increased aggression pushes them to train more intensely and be more assertive during competition and workouts.10 Anabolic steroids can be taken orally, transdermally, or intravenously. Most users take 5 to 10 times the physiologic dose, and some athletes admit using up to 100 times the physiologic amount.11
Human growth hormone has garnered media attention in professional sports, and research has shown use by high school students looking to improve their athletic performance.17 Its appeal has been linked to decreasing subcutaneous fat resulting in a more toned appearance. Because HGH also causes fluid shifts in the body soon after use, this reinforces the idea that the athlete is getting effects quickly, another appealing feature for adolescents.


Antiestrogen use has been discussed among college and professional athletes, yet there is little evidence of use in younger athletes. These increase levels of androgens in the blood by blocking the conversion of androgens to estrogens.
Blood doping is another performance-enhancing practice. Various methods exist, all of which increase the number of red blood cells in the bloodstream and artificially increase the blood’s ability to deliver oxygen to skeletal muscles.12 The most popular forms are injected erythropoietin and red blood cell transfusion. Blood doping increases endurance and stamina. It has been used in endurance sports such as cycling, distance running, and swimming.
Caffeine and stimulants (eg, amphetamine and methylphenidate) are banned substances that are common in popular culture as well as in the sporting arena.9,10,12 Caffeine shows ergogenic (performance-enhancing) properties at high doses (3-6 mg/kg). Athletes and nonathletes use stimulants, easily found in energy drinks, OTC supplements, alternative medications, and soft drinks, to stimulate the central nervous system, increase focus and energy, and work out longer. Caffeine, ephedrine, guarana, and ephedra alkaloids (eg, Ma Huang) are widely available. Effects are variable, however, and more research is needed to know the extent of the impact on children and adolescents.
NEXT: How to manage young athletes
Management
Open communication is essential to understanding what young athletes are doing to improve their appearance and performance. It is also important for finding out what they may be considering. This is an opportunity to educate and guide them to make safe and knowledgeable choices. After all, the pressure to succeed, to win, to get stronger, and to make it to the next level can be all consuming. Although some families will reach out to their pediatrician for guidance, many families (and kids on their own) will be drawn to the “quick fix” that promises to transform the athlete into someone who is “bigger, better, faster, and stronger.” Advertisements glorify the possible effects of these substances, but the young athlete’s safety is not typically the focus. Guidance needs to be provided when young athletes struggle between the desire to “win at all costs” and the drive to do the right thing.
Next: A cautionary note on rest or withdrawal following a concussion
A well-directed interview and exam need to be used for screening. Incorporating questions into the preparticipation physical interview is one way to address these issues as part of a more casual/nonassuming conversation.18 In addition to interviewing the young athlete, there is also a need to address the parents about their observations, intentions for use/training styles, and concerns. It is important to ask in the same tone as other screening questions, such as those inquiring about a history of asthma, concussion, or family heart disease.12
Examples of screening questions could include:11,12,18
o Do you use anything to help you in sports or competition?
o Do you take any herbs, vitamins, or natural medicines?
o What is your typical training routine? Do you use anything to help improve your workouts (such as muscle recovery drinks, medicines)?
o Do you take any supplements to help your appearance or workouts?
o What do you typically drink to hydrate during the day? Do you use energy drinks or protein/nutrition shakes?
o Is there anything kids at school are using to get an edge?
Educational programs have been designed to teach students about the facts and myths of PES and nutrition.18,19 Research has shown that open dialogue and talking about these topics is more effective than simply providing written handouts. Children who have had discussions with teachers or providers are less likely to use supplements and steroids, and they are more likely to retain the new information.19
Pediatricians are the primary contact for many adolescents, and even their parents, within the medical community. As the number of children involved in sports and activities increases and the competition stiffens, more and more athletes and families are looking for ways to gain an advantage. Year-round training, early sports specialization, personal training, and travel teams are just part of the puzzle. Advances in sports nutrition and use of PES are an added challenge as providers aim to provide comprehensive care and guidance. The pediatric medical community needs to be actively involved, having knowledge of substances being used, educating families in an approachable, noncritical manner, and having an open dialogue with children during visits.
REFERENCES
1. Merkel DL. Youth sport: positive and negative impact on young athletes. Open Access J Sports Med. 2013;4;151-160.
2. Castillo EM, Comstock RD. Prevalence of use of performance-enhancing substances among United States adolescents. Pediatr Clin North Am. 2007;54(4):663-675.
3. American College of Sports Medicine, American Dietetic Association, Dietitians of Canada. Joint Position Statement: nutrition and athletic performance. American College of Sports Medicine, American Dietetic Association, and Dietitians of Canada. Med Sci Sports Exerc. 2000;32(12):2130-2145.
4. Nisevich PM. Sports nutrition for young athletes: vital to victory. Today’s Dietitian. 2008;10(3):44.
5. Spear BA. Nutrition management of the child athlete. In: Nevin-Folino NL. Pediatric Manual of Clinical Dietetics. 2nd ed. Chicago, IL: American Dietetic Association; 2003.
6. Meyer F, O’Connor H, Shirreffs SM; International Association of Athletics Federations. Nutrition for the young athlete. J Sports Sci. 2007;25(suppl 1):S73-S82.
7. American College of Sports Medicine, Sawka MN, Burke LM, et al. American College of Sports Medicine position stand. Exercise and fluid replacement. Med Sci Sports Exerc. 2007;39(2):377-390.
8. Black J. Should drinks like Gatorade sport the ‘junk food’ label? Washington Post. September 26, 2007:A01. http://www.washingtonpost.com/wp-dyn/content/article/2007/09/25/AR2007092502281.html. Accessed July 10, 2015.
9. Committee on Nutrition and the Council on Sports Medicine and Fitness. Sports drinks and energy drinks for children and adolescents: are they appropriate? Pediatrics. 2011;127(6):1182-1189.
10. Gomez J; American Academy of Pediatrics Committee on Sports Medicine and Fitness. Use of performance-enhancing substances. Pediatrics. 2005;115(4):1103-1106.
11. Calfee R, Fadale P. Popular ergogenic drugs and supplements in young athletes. Pediatrics. 2006;117(3):e577-e589.
12. Koch JJ. Performance-enhancing: substances and their use among adolescent athletes. Pediatr Rev. 2002;23(9):310-317.
13. Supreme Court of the United States. Vernonia School District 47J, Petitioner v Wayne Acton, et ux, etc. (94-590) 515 US 646. June 26, 1995.
14. Dietary Supplement Health and Education Act of 1994. Public Law No. 103-417. October 25, 1994.
15. Greydanus DE, Patel DR. Sports doping in the adolescent: the Faustian conundrum of hors de combat. Pediatr Clin North Am. 2010;57(3):729-750.
16. Grunbaum JA, Kann L, Kinchen S, et al. Youth risk behavior surveillance-United States, 2003. MMWR Surveill Summ. 2004;53(2):1-96.
17. Rickert VI, Pawlak-Morello C, Sheppard V, Jay MS. Human growth hormone: a new substance of abuse among adolescents? Clin Pediatr (Phila). 1992;31(12):723-726.
18. Holland-Hall C. Performance-enhancing substances: is your adolescent patient using? Pediatr Clin North Am. 2007;54(4):651-662.
19. Goldberg L, MacKinnon DP, Elliot DL, Moe EL, Clarke G, Cheong J. The adolescents training and learning to avoid steroids program: preventing drug use and promoting health behaviors. Arch Pediatr Adolesc Med. 2000;154(4):332-338.
Dr Frye serves as teaching faculty for the Michigan State University College of Human Medicine, East Lansing. She also is a nonsurgical pediatric orthopedics and sports medicine physician in Grand Blanc, Michigan. The author has nothing to disclose in regard to affiliations with or financial interests in any organizations that may have an interest in any part of this article.

















