





A rare congenital anomaly
Diagnosis and treatment of congenital midline cervical cleft.
» What's the diagnosis?
» How would you treat her?


Diagnostic work-up included thyroid function tests, a thyroid scan, and a CT scan of the neck. Thyroid function tests were normal. Thyroid scan showed normal gland and no ectopic thyroid. CT scan showed linear density extending from posterior aspect of the skin tab to the isthmus of the thyroid gland, raising the suspicion of a sinus tract.
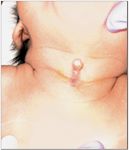
Diagnosis: Congenital midline cervical cleft
Congenital midline cervical cleft (CMCC) is a rare anomaly of the head and neck.1 It presents classically with atrophic midline vertical cleft in the anterior neck, with a cephalic hood-like skin tab and a caudal sinus.2-4 There have been fewer than 35 cases reported in the English-language literature, mostly in Caucasians.5,6
Serous fluid weeping in the early neonatal period is a common presentation, with gradual resolution of drainage over the next several months. Bulging of the neck and sternal region during straining is another clinical feature of CMCC.7 The area of the defect eventually heals as a widened scar, and is accompanied by a cord of subcutaneous tissue.8 This forms contracture of the neck with limitation of neck movements. If severe, the chin may be held in position of flexion.
Associated clinical features include cleft mandible, cleft lip, mandibular spurs, thyroglossal cyst, and rarely bronchogenic cyst or respiratory epithelium.9 Associated stapedial fixation has been reported, leading to bilateral conductive deafness.5
Pathogenesis
In Tessier's classification, CMCC is described as a variant of No. 30 facial cleft without any major bony defect.10 Several mechanisms have been proposed to explain midline cervical clefting, but the embryopathogenesis of the anomaly has not been clearly established. The most commonly accepted explanation is an impaired fusion of the distal branchial arches in the midline.7
Another proposed mechanism is increased pressure on the cervical area from the pericardial roof in early stages of the developing embryo.2 According to Bergevin et al, the vertical cleft may represent a persistent mucosal surface of either ectodermal or endodermal origin, similar to the vermilion surface of the lip. The skin projection represents the vertical outgrowth of tongue musculature, and the fibrous cord is related to the internal fibrous septum of the tongue base.4
Treatment
The patient underwent surgical exploration of the cleft. No sinus tract from the cleft to thyroid gland was identified. The skin tab and cervical cleft was excised uneventfully. Cytopathology of the surgical specimen showed fibrofatty and skeletal tissue beneath the skin. Early excision is the treatment of choice to prevent contracture of the neck, and for cosmetic improvement. It is important that all pathologic tissue in the midline is removed, to prevent development of contracture.3 Excision should be performed using a z-plasty repair in order to avoid a vertical scar, and subsequent cicatricial contracture.3










Recognize & Refer: Hemangiomas in pediatrics
July 17th 2019Contemporary Pediatrics sits down exclusively with Sheila Fallon Friedlander, MD, a professor dermatology and pediatrics, to discuss the one key condition for which she believes community pediatricians should be especially aware-hemangiomas.





