





The sex-trafficked child
Children can be victims of sex trafficking without ever leaving home, and it is almost certain that pediatricians are encountering trafficked victims every day without realizing it.
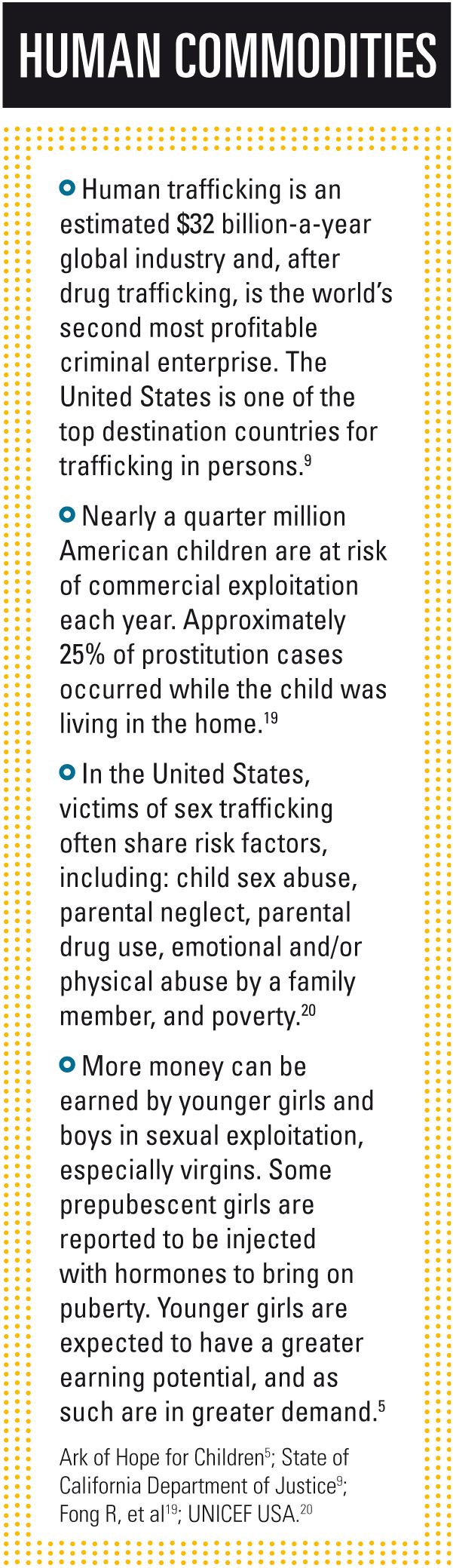
Child sex trafficking is some dark, nefarious atrocity that occurs in other places, on the other side of the world. At least, that’s what we’d like to believe. The sad truth is that human trafficking-specifically, child sex trafficking-is a thriving industry, one very thoroughly ensconced in the United States. Approximately 100,000 children are trafficked in the United States annually.1
The Victims of Trafficking and Violence Protection Act of 2000 (TVPA, PL 106-386) defines this activity as “‘sex trafficking in which a commercial sex act is induced by force, fraud, or coercion, or in which the person induced to perform such act has not attained 18 years of age . . . .’ Experts generally agree that the trafficking term applies to minors whether the child’s actions were forced or appear to be voluntary.”2
Jordan Greenbaum, MD, medical director, Stephanie Blank Center for Safe and Healthy Children, Children’s Healthcare of Atlanta Child Protection Center, Georgia, says, “Victims don’t choose their lifestyle with any kind of ‘informed consent.’ They are manipulated, betrayed, and deluded by adults far more savvy than they. They truly are victims, rather than ‘bad kids’ who choose their life, and they are not ‘offenders.’”
Aimee Grace, MD, MPH, works with the Stanford Advocacy Track Human Trafficking and Healthcare Project, Stanford University School of Medicine, California, and explains that awareness-or lack thereof-complicates the problem. “Community pediatricians should know that human trafficking is not just an international problem,” Grace says. “It is very real in our American communities.”
Greenbaum believes that many pediatricians encounter trafficked children without realizing it. “This is not something that simply happens abroad, or only involves foreign victims,” she says. “Most of the victims we see are US citizens.”
Detra West, BS, MS, a sociologist, associate dean of students and director of diversity and inclusion at Hiram College, Hiram, Ohio, agrees. “There’s a complete network of individuals from every walk of life who are involved in this,” says West, who teaches courses in human trafficking at the college. “We’re not just talking about the Big Bad Wolf. We’re talking about people we work with, perhaps. People who are abolitionists, who claim to be against it, can be participating in it.”
Get Contemporary Pediatrics for FREE in your Inbox
The trafficked child
Child trafficking victims are usually recruited and exploited in prostitution by family members, friends, and strangers, as well as by traffickers/pimps who pose as



“boyfriends.” Although many victims are young people in the child welfare system and/or runaways, some are recruited from middle-class families. These trafficked children may have a history of physical and sexual abuse in the home or be trafficked and sold for sex by a drug-addicted parent. A child can be a victim of sex trafficking without ever leaving his or her home.3
Runaways or children in foster care are also very vulnerable “because they are already in the system and can be used and abused this way, and no one questions it,” West says. “Most kids in foster care are there for a reason, because they have been in situations already of neglect, abuse, physical abuse. If a child is exhibiting problems, maybe issues in school, people automatically dismiss it-‘well, that’s a foster child, so he or she has problems anyway.’”
Greenbaum says pediatricians should be vigilant, and knowing some of the risk factors helps to determine when additional screening needs to occur. Risk factors can include:
- runaway/throwaway status;
- history of abuse/neglect;
- history of dysfunctional family;
- poverty;
- mental health problems; and
- drug-use problems.


However, physicians should avoid tunnel vision, because, “of course, not all kids have [discernible] risk factors,” Greenbaum points out.
In many cases, parents are selling their own children and the children never leave the home or their parents’ custody, West says.
Statistics may underestimate the number of familial traffickers. Potentially, as many as 30% of domestically trafficked minors who receive services through WestCare Nevada, a Las Vegas-area shelter for at-risk youth, are exploited by family members. When Shared Hope International aligned with US Department of Justice-funded human trafficking task forces to assess domestic minor sex trafficking in 10 US locations, interviewees from all 10 locations recounted cases in which parents or guardians acted as traffickers.3,4 Data collected by the National Center for Missing and Exploited Children (NCMEC) indicate that 69% of identified child pornography victims were abused and/or exploited by people familiar to the children, including parents, other relatives, neighbors, friends, babysitters, or guardians’ partners.1
Although many sources say most victims are first trafficked between the ages of 12 and 14 years,1,5-7 West says victims often start much younger-from 3 to 8 years, an age cited by trafficking-awareness organizations such as Dosomething.org and traffickinghope.org.
Identifying the child victim
Identifying and rescuing the victims are complicated by the complexity of sex trafficking networks, methods of control imposed by traffickers, and the challenges victims face in seeking assistance.
Aggravating the situation, Grace notes, is that community pediatricians are very likely seeing child trafficking victims “but may not be aware of it,” she says, adding victims may face many atrocities, including labor and sexual trafficking. “Some people believe that if you don’t see human trafficking, it’s because you’re not looking for it,” Grace says.
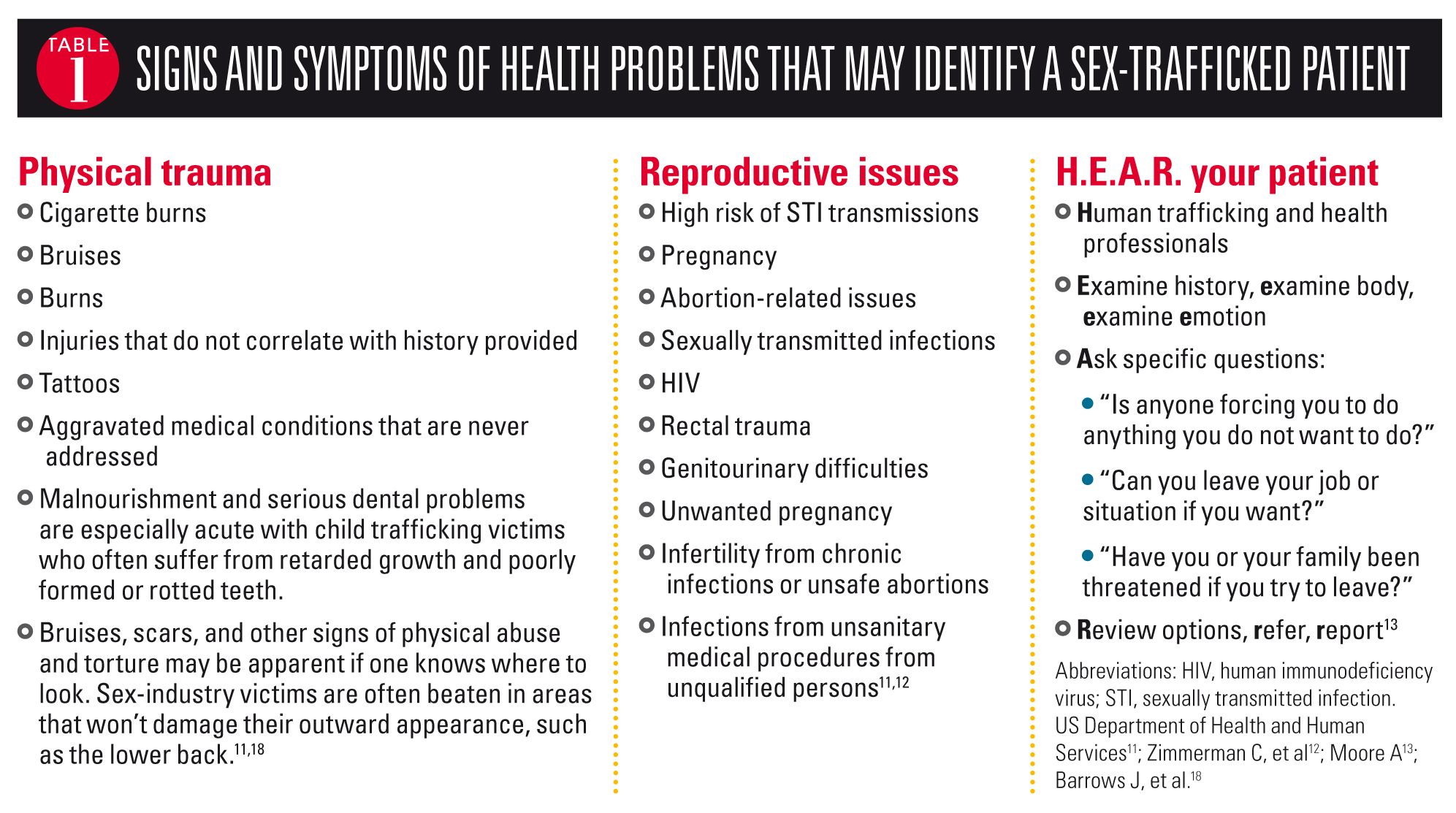
Yet such victims are everywhere. They live at home with their parents or foster families, and it’s almost certain that physicians and others within the healthcare industry are encountering them.8 There are indicators, clinical and otherwise, that pediatricians and other healthcare providers may observe (Table 1).


Traffickers will often tattoo children,9 typically on the neck or a little symbol on the shoulder. Because children aren’t legally permitted to receive tattoos before the age of 18 years, any such mark should be an immediate red flag to healthcare providers. “That is a clear indication that someone is trafficking this child,” West says. “The trick for the physician is to talk directly to the child. Even if the parent wants to answer all the questions, the conversation needs to involve the child. Typically, the child will sound rehearsed. The eyes will dart to the parent to get approval. Some of that’s normal.”
Grace says there are things pediatricians should avoid doing so as not to further endanger a child. “A pediatrician should avoid terms such as ‘human trafficking victim’ as this will likely have no meaning for the child/adolescent,” she says.


Greenbaum agrees, adding that the person accompanying the child may be the trafficker or tell the trafficker what the child says. “That can endanger the child and/or her family. The pediatrician should take steps to make sure the conversation is private, uninterrupted, and that the child feels safe,” she says. Then asking specific questions-such as history of sexually transmitted infections, age of boyfriends, pregnancies, number of sex partners, history of abuse or drug use-can provide very revealing information.
“And in cases in which the pediatrician is suspicious,” Greenbaum says, “the physician may want to ask direct questions, such as: ‘Has anyone ever asked you to have sex with someone else?’ or ‘Have you ever had to exchange sex for something you needed or wanted?’”
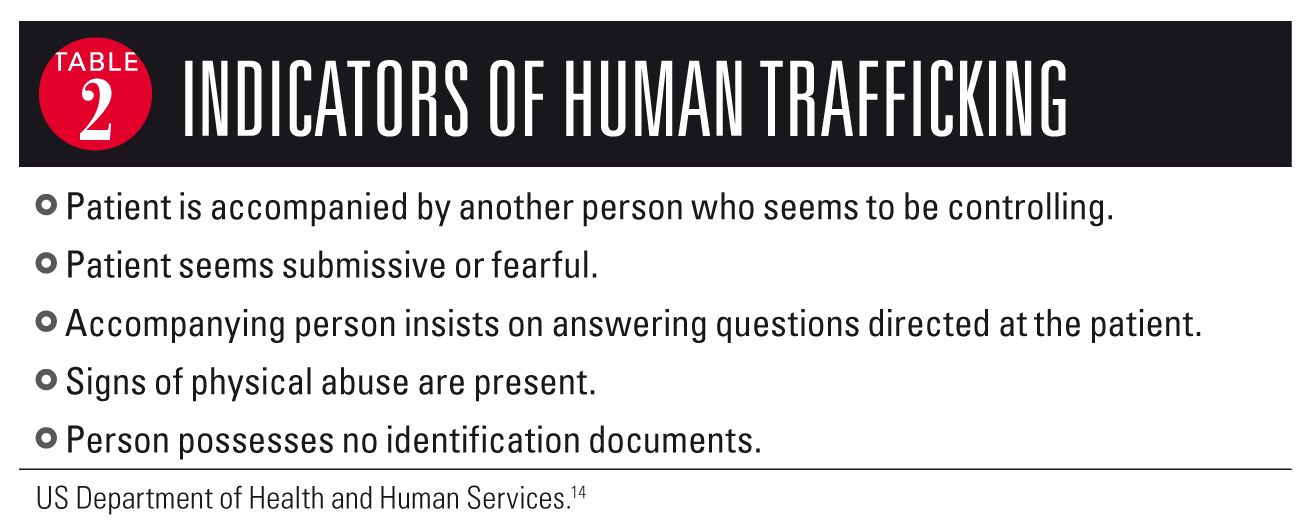
Grace says physicians can learn to identify a trafficked patient (Table 2), and she refers to the US Department of Health and Human Services Office of Refugee Resettlement as a good resource. The Rescue and Restore Victims of Human Trafficking Campaign Tool Kits provide a wealth of information, including tips for identifying and assisting victims, screening questions, the trafficking victims’ mindset, communicating with human trafficking victims, health problems seen in trafficked victims, and resources such as PowerPoint presentations, posters, and brochures for healthcare providers.10


A physical exam will often yield evidence of the victim being controlled.11-13 He or she may exhibit bruises or other signs of battering and have fear or depression. Urinary tract or bladder infections in girls, especially recurring bladder infections, can be an indication of possible abuse, as are sexually transmitted diseases, HIV/AIDS, pelvic pain, and rectal trauma. Malnourishment, retarded growth, and poorly formed or rotted teeth are especially acute with pediatric trafficking victims. Bruises, scars, and other signs of physical abuse may be apparent in areas that won’t damage victims’ outward appearance, such as the lower back.
Treatment and care paths often differ for a trafficked child compared with a victim of more typical domestic abuse. For the trafficked victim, the psychological ramifications of being owned, of being someone else’s property, can create overwhelming psychosocial hurdles. From a physical standpoint, the victim has often received insufficient healthcare or medical attention.11 West notes that when a trafficker seeks treatment for a child, he or she is seeking not so much care as cure. He or she wants the child cured so that child can return to making money. This cure versus care mentality may translate to lack of follow-up, failure to comply with treatment recommendations, and ultimately long-term physical and psychiatric complications for the child.14
Grace says pediatricians should know that there are many legal resources available to help victims of trafficking, based on the Victims of Trafficking and Violence Protection Act of 2000.15 West adds that in situations where a physician reports suspected abuse, the authorities bring in others to take over. So, the pressure isn’t on the pediatrician to know all the symptoms with which a trafficked child may present.16
Reporting is imperative
Grace recommends, “Pediatricians should refer to Child Protective Services if the child is under 18; for those 18 and older, pediatricians must observe confidentiality, but can encourage the victim to report the crime.”


Is it possible for a trafficked child to eventually grow up and have some semblance of a normal life?
“Surviving all that, coming through all that, and having some form of recovery, that’s the best possible outcome,” West says. “Can a person walk away from that kind of abuse and end up perfectly normal? I don’t know. I think most psychologists would say they’ll be [posttraumatic stress disorder] victims.”
While trafficked children experience a different abuse model than “typically” abused children, without intervention and effective treatment (physical and psychological), both groups may evolve from abused children into adults who abuse.7,17 Removing a child from a trafficking situation may save future generations by interrupting the cycle.
That’s where community pediatricians can make a difference, Grace notes. “Let me add what pediatricians should do. Call a social worker, call the National Human Trafficking Hotline (888-373-7888), and call 911 if there is urgent danger. Pediatricians should also establish a relationship of trust, remind victims of their legal rights, and assure the victims that they are there to help.”
Greenbaum concurs. “Exploited youth have immense needs and the pediatrician should reach out to other organizations for help,” she says. “No one can do it alone.”





REFERENCES
1. National Center for Missing and Exploited Children. http://www.missingkids.com/home. Accessed February 28, 2014.
2. Finklea M, Fernandes-Alcantara AL, Siskin A. Sex Trafficking of Children in the United States: Overview and Issues for Congress. Congressional Research Service, 7-5700, R41878. Available at: http://www.fas.org/sgp/crs/misc/R41878.pdf. Published June 21, 2011. Accessed February 28, 2014.
3. Domestic Minor Sex Trafficking. In: Smith L, Healy Vardaman S, Snow M. The National Report on Domestic Minor Sex Trafficking: America’s Prostituted Children. Vancouver, WA: Shared Hope International; 2009;4-15.
4. Kennedy MA, Pucci NJ. Domestic Minor Sex Trafficking: Las Vegas, Nevada. Vancouver, WA: Shared Hope International; 2008;106.
5. Ark of Hope for Children. Child trafficking statistics, U.S. and international. Available at: http://www.arkofhopeforchildren.org/child-trafficking/child-trafficking-statistics. Updated February 22, 2014. Accessed February 28 2014.
6. Hammer H, Finkelhor D, Sedlak AJ. National Incidence Studies of Missing, Abducted, Runaway, and Thrownaway Children: Runaway/Thrownaway Children: National Estimates and Characteristics. Available at: https://www.ncjrs.gov/pdffiles1/ojjdp/196469.pdf. Published October 2002. Accessed February 28, 2014.
7. Vulnerability. In: Smith L, Healy Vardaman S, Snow M. The National Report on Domestic Minor Sex Trafficking: America’s Prostituted Children. Vancouver, WA: Shared Hope International; 2009;30-36.
8. Family Violence Prevention Fund. Turning Pain into Power: Trafficking Survivors’ Perspectives on Early Intervention Strategies. San Francisco, CA: Family Violence Prevention Fund; 2005.
9. State of California Department of Justice, Office of the Attorney General. Human trafficking. Available at: http://oag.ca.gov/human-trafficking. Accessed February 28, 2014.
10. US Department of Health and Human Services, Office of Refugee Resettlement. Rescue and Restore Campaign Tool Kits. Available at: http://www.acf.hhs.gov/programs/orr/resource/rescue-restore-campaign-tool-kits. Published July 23, 2012. Accessed February 28, 2014.
11. US Department of Health and Human Services, Office of Refugee Resettlement. Rescue and Restore Campaign Tool Kits. Resources: Identifying and interacting with victims of human trafficking. Available at:
http://www.acf.hhs.gov/sites/default/files/orr/tips_for_identifying_and_helping_victims_of_human_trafficking.pdf. Accessed February 28, 2014.
12. Zimmerman C, Yun K, Watts C, et al. The Health Risks and Consequences of Trafficking in Women and Adolescents. Findings from a European Study. London: London School of Hygiene and Tropical Medicine, 2003. Available at: http://www.oas.org/atip/Global%20Reports/Zimmerman%20TIP%20HEALTH.pdf. Accessed February 28, 2014.
13. Moore A. An Intervention Mapping Approach: Identification of Human Trafficking Victims by Health Professionals [master’s thesis]. Houston, Texas: University of Houston School of Public Health; 2010.
14. US Department of Health and Human Services, Office of Refugee Resettlement. Rescue and Restore Campaign Tool Kits. Look Beneath the Surface: Role of Health Care Providers in Identifying and Helping Victims of Human Trafficking [PowerPoint]. Available at: http://www.acf.hhs.gov/programs/orr/resource/rescue-restore-campaign-tool-kits. Published July 23, 2012. Accessed February 28, 2014.
15. Victims of Trafficking and Violence Protection Act of 2000. Public Law 106-386. October 28, 2000. Available at: http://www.state.gov/documents/organization/10492.pdf. Accessed February 28, 2014.
16. Isaac R, Solak J, Giardino AP. Health care providers’ training needs related to human trafficking: maximizing the opportunity to effectively screen and intervene. J Appl Res Children. 2011;2(1):1-32.
17. Network of Victim Assistance. Child sexual abuse. Available at: http://www.novabucks.org/otherinformation/childsexualassault/. Accessed February 28, 2014.
18. Barrows J, Finger R. Human trafficking and the healthcare professional. South Med J. 2008;101(5):521-524.
19. Fong R, Cardoso JB. Child human trafficking victims: challenges for the child welfare system. Eval Program Plann. 2010;33:311-316.
20. UNICEF USA. End Trafficking ToolKit. Available at: http://www.unicefusa.org/campaigns/end-trafficking/. Accessed February 28, 2014.
21. US Department of State, Human Smuggling and Trafficking Center. Fact Sheet: Distinctions Between Human Smuggling and Human Trafficking. Available at: http://2001-2009.state.gov/g/tip/rls/fs/2005/57345.htm. Published January 1, 2005. Accessed February 28, 2014.
22. Estes RJ, Weiner NA. Commercial Sexual Exploitation of Children in the U.S., Canada, and Mexico. Philadelphia, PA: University of Pennsylvania; 2001:60.
Ms Donley-Hayes, BA, MA, MFA, is a medical writer and editor in Ohio. She has nothing to disclose in regard to affiliations with or financial interests in any organizations that may have an interest in any part of this article.

















