





Dispel the myth, save the child
Baby teeth are vitally important. It’s time we made their protection a North American public health priority.
Early childhood caries (ECC) once was known as baby bottle tooth decay. Among its causes were poor nutrition, a lack of basic dental care, and extended exposure of the teeth to sugars-often when babies were put to bed with bottles containing milk, formula, and fruit juice. Although known to be preventable, bottle decay was considered by many dental and medical professionals to be a normal part of childhood and a relatively harmless affliction to baby teeth-teeth that were going to fall out on their own once adult teeth emerged.
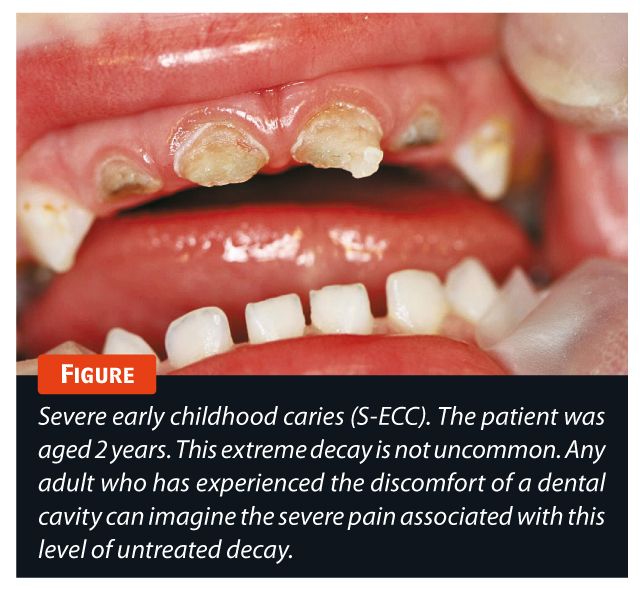
In truth, ECC is extraordinarily dangerous and destructive. It is the number one chronic, infectious disease in children aged 5 years and younger in North America.1 The condition is defined as the presence of decayed teeth or missing teeth due to decay; acute cases in children aged younger than 3 years are referred to as severe early childhood caries (S-ECC; Figure 1).2


The US National Center for Health Statistics reports that ECC afflicts 28% of North American children aged between 2 and 5 years-about 5 million kids. Approximately 1.2 million (23%) of these children never receive treatment.3,4 The disease is epidemic among many minority, immigrant, rural, and remote populations.4,5 Some research estimates the incidence of ECC in Aboriginal children is greater than 70%. In 2001 alone, more than 6,000 Aboriginal children under age 5 in Canada had all their upper front teeth removed due to dental disease.6
Advances in dental care and public awareness have failed to reduce the incidence of ECC and S-ECC in North America. While dental associations in both Canada and the United States have recognized the seriousness of the problem, many dentists do not see the need to treat patients under the age of 3 years, even though current practice guidelines recommend that first dental visits should occur as early as 6 months of age and no later than 12 months.
The myth prevails
Today, the myth prevails among professionals and the public: Baby teeth are expendable; they’ll be lost eventually, so why spend money on their protection?
The price of their loss makes for perhaps the most compelling reason. ECC-related dental surgery under general anesthesia is the single most common surgical procedure at most pediatric hospitals in Canada.7,8 According to the Canadian Institute for Health Information, “The roughly 19,000 day surgery operations for children younger than age 6 each year pose potential health risks to children and can be traumatic for both children and their families.”8
Numerous studies point to the relationship between ECC or S-ECC and iron deficiency, iron deficiency anemia,9,10 protein deficiencies (albumin), vitamin D deficiency,11-13 and increased salivary cortisol levels.14
Children with ECC and S-ECC experience debilitating pain that impedes sleep, good nutrition, and overall development-in some cases, for years. When treatment is delayed or denied, children with ECC endure toxic stress, which is the experience of powerful, frequent, or prolonged suffering. Toxic stress dramatically alters brain development in children. It’s been linked to poor impulse control, mood control problems, learning disabilities, and impaired memory.15
This profound level of stress may be equivalent to recurrent abuse and chronic neglect.16 Indeed, research shows a correlation between child abuse and neglect and the incidence of ECC and S-ECC.16-22 Abused and neglected children grow up to become adults who suffer significantly higher rates of obesity, type 2 diabetes, cardiovascular disease, hypertension, anxiety disorders, addictive behaviors, and suicide.23 In many jurisdictions, the failure to report observed cases of neglect compels authorities to levy charges.
So what does this legal obligation mean for parents who put their babies to bed with bottles of sugar-filled liquids? What does it mean for a pediatrician who tells parents to see a dentist about their baby’s dental issues? What does it mean for a dentist who refuses to see young patients simply because they are not yet 3 years old?
It means we all need to acknowledge ECC as a serious public health problem.
Western health care has evolved to assign the treatment of teeth to dentists and the treatment of the rest of the body to physicians. ECC has thrived in this disciplinary divide and underscores the need to treat patients holistically. The mouth is a gateway to the body; the health of one is inextricably tied to the well-being of the other. As an infectious disease, ECC can spread throughout the body to affect other organs. For example, untreated, the disease has led to brain abscesses that require costly and complex surgical intervention and has sometimes proved fatal.24-26
Prevention is the best treatment
ECC prevention is simple and inexpensive. The solution is a coordinated and actively promoted campaign to boost awareness throughout North America. To succeed, the campaign must engage medical and dental associations and professionals, social workers, insurance bodies, health care organizations, and public health authorities at all levels. In the true spirit of collaboration, their goal should be to develop an ongoing, multiplatform, public education program that:
- acknowledges dental disease as a serious medical condition;
- stresses the need for all children to have their first dental visit at 6 months of age but no later than 12 months;
- promotes proper prenatal and perinatal nutrition;
- teaches parents the simple procedures for cleaning the teeth of even the youngest children27; and that
- familiarizes children with the ease of cleaning and the importance of healthy teeth.
Together, we must work to integrate infant medical and dental care to explore correlations between oral health and physiological development. To stem the spread of ECC and diminish its current impact, we must also seize opportunities to provide low-cost or free dental consultation services to low-income citizens and those who live in remote communities.
The benefits of this campaign are obvious. The sooner we all make ECC a priority, the sooner we will slash related health care costs, dramatically reduce the number of ECC cases, and eliminate the lasting effects of this debilitating and totally preventable disease.
REFERENCES
1. Drury TF, Horowitz AM, Ismail AI, et al. Diagnosing and reporting early childhood caries for research purposes. A report of a workshop sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health and Financing Administration. J Public Health Dent. 1999;59;192-197.
2. American Academy of Pediatric Dentistry. Early childhood caries (ECC): classifications, consequences, and preventive strategies. Pediatr Dent. 2012;34(6):50-52.
3. Dye BA, Tan S, Smith V, et al. Trends in oral health status: United States, 1988-1994 and 1999-2004. Series 11, No. 248. Washington, DC: National Center for Health Statistics; 2007.
4. Edelstein BL. The dental caries pandemic and disparities problem. BMC Oral Health. 2006;6 suppl 1:S2.
5. Hobdell MH, Oliveira ER, Bautista R, et al. Oral diseases and socio-economic status (SES). Br Dent J. 2003;194(2):91-96.
6. Lawrence HP, Romanetz M, Rutherford L, Cappel L, Binguis D, Rogers JB. Probe. 2004;38(4):172-190.
7. Canadian Dental Association. CDA position on early childhood caries. http://www.cda-adc.ca/_files/position_statements/earlyChildhoodCaries.pdf. Approved April 2010. Accessed December 9, 2013.
8. Canadian Institute for Health Information. Treatment of Preventable Dental Cavities in Preschoolers: A Focus on Day Surgery under General Anesthesia. Ottawa, ON: CIHI;2013. https://secure.cihi.ca/estore/productFamily.htm?locale=en&pf=PFC2386&lang=en. Accessed December 9, 2014.
9. Schroth RJ, Levi J, Kliewer E, Friel J, Moffatt ME. Association between iron status, iron deficiency anaemia, and severe early childhood caries: a case-control study. BMC Pediatr. 2013;13:22.
10. Mobley C, Marshall TA, Milgrom P, Coldwell SE. The contribution of dietary factors to dental caries and disparities in caries. Acad Pediatr. 2009;9(6):410-414.
11. Taylor GF, Day CD. Dental caries, vitamin D, and mineral deficiencies. Br Med J. 1939;1(4087):919-921.
12. Hujoel PP. Vitamin D and dental caries in controlled clinical trials: systematic review and meta-analysis. Nutr Rev. 2013:71(2);88-97.
13. Schroth RJ, Levi JA, Sellers EA, Friel J, Kliewer E, Moffatt ME. Vitamin D status of children with severe early childhood caries: a case-control study. BMC Pediatr. 2013;13(1):174.
14. Boyce WT, Den Besten PK, Stamperdahl J, et al. Social inequalities in childhood dental caries: the convergent roles of stress, bacteria and disadvantage. Soc Sci Med. 2010;71(9):1644-1652.
15. Shonkoff JP, Garner AS; Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics. The lifelong effects of early childhood adversity and toxic stress. Pediatrics. 2012;129(1):e232-e246.
16. Nuzzolese E, Lepore M, Montagna F, et al. Child abuse and dental neglect: the dental team’s role in identification and prevention. Int J Dent Hyg. 2009;7(2):96-101.
17. Blumberg ML, Kunken FR. The dentist’s involvement with child abuse. N Y State Dental J.1981;47(2):65-69.
18. Hendler TJ, Sutherland SE. Domestic violence and its relation to dentistry: a call for change in Canadian dental practice. J Can Dent Assoc. 2007;73(7):617.
19. Valencia-Rojas N, Lawrence HP, Goodman D. Prevelance of early childhood caries in a population of children with a history of maltreatment. J Public Health Dent. 2008;68(2):94-101.
20. Rupp RP. Conditions to be considered in the differential diagnosis of child abuse and neglect. Gen Dent. 1998;46(1):96-100.
21. Montecchi PP, Di Trani M, Sarzi Amadè D, Bufacchi C, Montecchi F, Polimeni A. The dentist’s role in recognizing childhood abuses: study on the dental health of children victims of abuse and witnesses to violence. Eur J Paediatr Dent. 2009;10(4):185-187.
22. Greene PE, Chisick MC, Aaron GR. A comparison of oral health status and need for dental care between abused/neglected children and nonabused/non-neglected children. Pediatr Dent. 1994;16(1):41-45.
23. Centers for Disease Control and Prevention. Adverse Child Experiences (ACE) study. http://www.cdc.gov/ace/. Updated January 18, 2013. Accessed December 9, 2013.
24. Azenha MR, Homsi G, Garcia ir Jr. Multiple brain abscess from dental origin: case report and literature review. Oral Maxillofac Surg. 2012;16(4):393-397.
25. Otto M. For want of a dentist. Washington Post. February 28, 2007. http://www.washingtonpost.com/wp-dyn/content/article/2007/02/27/AR2007022702116.html. Accessed December 10, 2013.
26. Hibberd CE, Nguyen TD. Brain abscess secondary to a dental infection in an 11-year-old child: case report. J Can Dent Assoc. 2012;78:c49.
27. American Academy of Pediatrics. A Pediatric Guide to Children’s Oral Health. Elk Grove Village, IL: American Academy of Pediatrics; 2009. http://www2.aap.org/oralhealth/docs/oralhealthfcpagesf2_2_1.pdf. Accessed December 10, 2013.



DR SMITH is a pediatric dentist and diplomate of the American Board of Pediatric Dentistry; clinical assistant professor, Department of Pediatrics, University of Calgary Faculty of Medicine, Canada; and chairman and CEO of the Society for a Healthy Mouth, Healthy Child (Alberta) and the Foundation for a Healthy Mouth, Healthy Child (United States), nonprofit charitable organizations dedicated to eradicating early childhood caries.

















