





PEDIATRIC PUZZLER
A 14-year-old is referred to your emergency department for evaluation of recurrent episodes of abdominal pain. Over the past year he has had five such episodes, separated by symptom-free intervals of about two months. The pain has been consistently periumbilical, without radiation or localization, and each of the five instances of pain has been associated with a bifrontal headache. The last episode before the present one, two months ago, was the first associated with fever.
PEDIATRIC PUZZLER
"Read my lips": Abdominal pain in a 14-year-old
Jonathan E. Teitelbaum, MD, Steven J. Fishman, MD, Alan M. Leichtner,MD, and Walter W. Tunnessen, Jr., MD
A 14-year-old is referred to your emergency department for evaluationof recurrent episodes of abdominal pain. Over the past year he has had fivesuch episodes, separated by symptom-free intervals of about two months.The pain has been consistently periumbilical, without radiation or localization.Each of the five instances of pain has been associated with a bifrontalheadache; nausea and vomiting have not been present, however. The last episodebefore the present one, two months ago, was the first associated with fever.The pain typically begins late at night or early in the morning and resolveswithin 24 hours.
On this occasion, the pain began when the adolescent awoke in the morning,about seven hours ago, and it is described, like the other episodes, asperiumbilical and severe enough to cause him to "double over."This time, though, there is no associated headache, and the young man complainsof nausea and has had emesis. As you obtain further history, the adolescentdescribes the pain as somewhat intermittent, lasting 10 minutes with a crescendo-decrescendopattern that is partially relieved by vomiting. Before coming to the EDhe has had emesis nine times, each nonbloody and nonbilious. He describeshaving normal daily bowel movements with no diarrhea. He denies recurrentfever, weight loss, joint aches, or eye complaints. The only reduction inappetite is the result of the present nausea. There has been no abdominaltrauma. He denies taking any medications and specifically denies drinkingalcohol. The parents report that his past medical history is unremarkable;he has had no surgery. No other family members are ill or have similar historiesof recurrent abdominal pain. The family history is noncontributory.
During the physical examination the young man has intermittent episodesof apparent pain. He is afebrile with a normal heart rate, respiratory rate,and blood pressure. His height and weight are appropriate, both betweenthe 50th and 75th percentiles. His sclerae are anicteric and the optic discsare flat. His mucous membranes are moist. The lungs are clear to auscultationand no murmurs are heard on cardiac examination. The abdomen is soft andnot distended. Only mild tenderness is apparent on palpation in the periumbilicalarea. There are no palpable masses or organomegaly and the bowel soundsare normoactive. Both testes are descended and nontender; no hernias arepresent. There is no evidence of perianal disease, and the rectal examinationis benign, without tenderness or masses. The stool is guaiac-negative. Theneurologic examination also appears normal, and the young man has no clubbing,cyanosis, or edema of the extremities, and no joint abnormalities. He hasno purpuric or petechial lesions on his skin. Only a few scattered frecklesare present on his forearms and lower lip.
Hammering out a differential diagnosis
The causes of abdominal pain are extensive; perhaps if the type of painis considered, the differential can be more focused. The pain appears tobe colicky, which may suggest disorders resulting in obstruction of a hollowviscus. The intestines would be the first organ to consider. Could thisbe small bowel obstruction? Adhesions could cause intermittent obstruction,but the young man has never had a surgical procedure, making this possibilityless likely. An incarcerated hernia may cause these symptoms, but nothingwas found on physical examination. An intra-abdominal hernia is much lesscommon. Inflammatory bowel disease? Crohn disease might produce these symptoms,but there is nothing to corroborate this hypothesis--no evidence of chronicinflammation, such as weight loss or fatigue; guaiac-negative stool; noextra-intestinal manifestations.
Could this be a volvulus from a previously undiagnosed intestinal malrotation?Volvulus can occur at any age, although it is certainly more common in thefirst few years of life. Intussusception can be recurrent and result insymptoms like this. Colonic obstruction from a fecal impaction is highlyunlikely given the normal bowel history, absence of mass on abdominal palpation,and negative rectal examination. What about appendicitis? Atypical presentationsabound, but the pain is usually constant and the tenderness more localized.
Should we consider obstruction of another viscus? What about cholelithiasisand obstruction of the biliary tree? Against a biliary problem are the lackof right upper quadrant pain, tenderness, and jaundice, and the absenceof risk factors for stone formation. Renal stones, similarly, should presenta somewhat different picture, although Dietl crisis--episodes of abdominalpain and vomiting associated with obstruction of the uretero-pelvic junctionfollowing increased urine production as a result of ingestion of large quantitiesof fluids--could produce a pattern like this.
Henoch-Schönlein purpura may be associated with colicky abdominalpain, particularly when intussusception is present, although this problemgenerally occurs in young children. No matter that there are no purpuriclesions; they may develop later in the course of the disease. Lactose intolerancecan cause recurrent, colicky abdominal pain, but the history does not fit.Nor do the presentations of duodenal or gastric ulcers, pancreatitis, andgastrointestinal infections or infestations.
The recurrent episodes and the history of headaches should not be forgotten.Could this be a manifestation of abdominal migraine? The young man's motherreports that she has intermittent headaches relieved by nonsteroidal anti-inflammatorydrugs, although her headaches have never been classified as migraine. Thiswill be a difficult diagnosis to nail to this youngster.
The possibilities continue to run through your brain as you plan a reasonedapproach to the evaluation of the problem.
Sounding out the cause
A CBC, obtained mainly to view the WBC count as a marker of inflammation,gives you pause. The WBC is 22,000/mL with a differential count of 90% polymorphonuclearcells and 5% band forms. The hematocrit is 42% and the platelet count isalso normal. Could this boy's pain be infection related? Liver transaminases,amylase, lipase, and electrolytes are normal, as is the urinalysis.
Supine and upright films of the abdomen are obtained. No suspicious calcifications(such as appendiceal fecalith, renal stones, or gallbladder stones) areseen. The bowel gas pattern is nonspecific, showing no distention of intestineor air-fluid levels, no unusual amount of stool in the colon or rectum,and no free air in the abdomen.
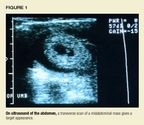
Perhaps an abdominal ultrasound will offer more help. The ultrasonographernotes what appears to be a midabdominal mass. A transverse scan shows atarget appearance that is most consistent with an intussusception, mostlikely ileo-ileal (Figure 1). The target appearance is formed as mesentericfat is sandwiched between proximal and distal bowel wall during intussusception.Using color Doppler, flow is identified to the intussusception.


Why intussusception and why were there no clues on the abdominal flatplate? Signs of intussusception on abdominal radiographs are mostly limitedto ileo-colic intussusception and include absence of cecal gas or stool,a crescent sign where air outlines the intussusception, soft tissue mass,inability to visualize the liver tip, and an interrupted gas column in thecolon.1,2 None of these signs is exclusive to intussusception,and studies show that plain radiographs will miss 33% to 50% of the diagnoses.Ultrasound, on the other hand, has been shown to have nearly 100% sensitivityin detecting intussusception in the hands of an experienced operator.1
The classic triad of signs and symptoms associated with intussusceptionare colicky abdominal pain, currant jelly or bloody stools (usually a latesign as intestinal mucosa is sloughed due to compromise of its vascularsupply), and an abdominal mass. This triad, unfortunately, is present inless than half the cases of intussusception.1
The incidence of intussusception is estimated at about 2.4 cases per1,000 children, and intussusception is the most common cause of intestinalobstruction in childhood.3 Recent epidemiologic studies recognizea bimodal distribution of cases with peaks at 5 months and 3 years of age.4In 90% of the cases the intussusception is ileo-colic and there is no identifiablelead point.1 Increasing age, however, greatly strengthens thelikelihood of a pathologic lead point.
Lead points for intussusception include structural abnormalities suchas Meckel diverticulum, ectopic gastric and pancreatic mucosa, inflamedappendix, appendiceal stump, and duplication cyst; vascular abnormalitiessuch as Henoch-Schönlein purpura, hemolytic-uremic syndrome, hematoma,and vascular malformation; neoplasms, including adenoma, lipoma, lymphoma,hamartoma, and sarcoma; and inflammatory lesions, foreign bodies (bezoars,sutures, ascaris, or feeding tubes), inspissated stool in cystic fibrosis,ileus, and celiac disease.3
What are the possibilities here? Were there any clues? What about thefreckles on the lips? (See Figure 2.) Is it possible that these were notsimple freckles but hyperpigmented macules as a clue to Peutz-Jeghers syndrome?



The young man is taken to the operating room where an irreducible intussusceptionis identified in the midsmall bowel. A 78-cm portion of the ileum isresected. Upon opening the resected specimen, four polyps are found, thelargest pedunculated and 3 cm in its largest dimension (Figure 3). Palpationof the remaining small bowel reveals another polyp, which is removed byenterotomy. Histological specimens demonstrate that the polyps are consistentwith Peutz-Jeghers hamartomas.



Paying lip service to the diagnosis
Back in 1896, Hutchinson described pigmentary changes of the lips andmouth in an individual who later died of intussusception. Peutz, in 1921,was responsible for classifying the disorder as one of the familial polyposissyndromes, and Jeghers, in 1949, further established the entity and thediagnostic significance of the hyperpigmented macules.5
Peutz-Jeghers syndrome is autosomal dominant in inheritance witha highdegree of penetrance. Recently the syndrome has been linked to the shortarm of chromosome 19, although no gene product has been identified to date.6
The syndrome is characterized by hyperpigmented macules, referred toas lip freckling, and intestinal hamartomas. Although freckling is commonin the normal population, the lips, buccal mucosa, and axillae are typicallyspared. The brown to black macules may be seen early in infancy on the lipsand they usually increase in intensity until puberty. Approximately 94%of patients with this syndrome have these hyperpigmented macules in theperioral region, 66% on the buccal mucosa, 74% on the hands, and 62% onthe feet.7 The spots on the lips may fade with time; however,the buccalmucosal lesions typically do not fade.
The intestinal hamartomas associated with Peutz-Jeghers syndrome havebeen found throughout the gastrointestinal tract from the esophagus to therectum, but they are most common in the small intestine. The polyps tendto be large and pedunculated with a firm, lobulated contour. Seventy percentof affected patients have some gastrointestinal problem by age 20 years,most commonly abdominal pain (60%), intestinal bleeding (25%), or both.5Some of the hamartomas progress to adenoma or carcinoma, although thesechanges are thought to occur in only 2% to 13% of patients.8
Interestingly, Peutz-Jeghers syndrome is associated with a high riskof extra-intestinal cancer, with as many as 40% being affected by 40 yearsof age.7 The cancers include sex cord tumors of the ovary in5% to 12% of females, feminizing Sertoli cell tumors of the testicle inmen, bronchogenic carcinoma, breast cancer, malignant adenoma of the cervix,thyroid cancer, pancreatic cancer, and bile duct cancer.7 Recommendationsfor the surveillance of affected individuals have not been universally accepted.The polyposis registry at St. Mark's Hospital in London has published recommendationsthat include endoscopy, both esophago-gastric-duodenal and colonoscopy,with polypectomy as needed, every other year. An upper gastrointestinalstudy with small bowel follow-through is also recommended every other year.Enterotomy with polypectomy is recommended for polyps 1.5cm or larger thatcannot be removed endoscopically. Women should undergo yearly pelvic ultrasonography,mammography, and Pap smears. Males should have yearly testicular examinationsand ultrasonography if they develop feminizing features.7
The differential diagnosis of abdominal pain is a large one, and thisis certainly not one of the common disorders associated with the complaint.However, we must always be alert to clues to help us in sorting throughthe possible causes. Stop, look, and listen. Sometimes the clue comes "outof the mouths of babes."
REFERENCES
1. Daneman A, Alton DJ: Intussusception: Issues and controversies relatedto diagnosis and reduction. Radiol Clin North Am 1996;34:743
2. Lazar L, Rathaus V, Katz S: Interrupted air column in the large bowelon plain abdominal film: A new radiological sign of intussusception. J PediatrSurg 1995;30:1551
3. Stringer MD, Pablot SM, Brereton RJ: Pediatric intussusception. BritJ Surg 1992;79:867
4. Lukis FI, Yazbeck S, Perreault G, et al: Changes in the presentationof intussusception. Amer J Emerg Med 1992;10:574
5. Peutz-Jeghers syndrome, in Jones KL (ed): Smith's Recognizable Patternsof Human Malformation, ed 5. Philadelphia, PA, WB Saunders Co, 1995, pp520521
6. Hemminki A, Tomlinson I, Markie D, et al: Localizatioin of a susceptibilitylocus for Peutz-Jeghers syndrome to 19p using comparative genomic hybridizationand targeted linkage analysis. Nat Genetics 1997;15:87
7. Spigelman AD, Arese P, Phillips RKS: Polyposis: The Peutz-Jegherssyndrome. Brit J Surg 1995;82:1311
8.Finan MC, Ray MK: Gastrointestinal polyposis syndromes. Dermatol Clin1989;7:419
DR. TEITELBAUM is a fellow in gastroenterology, Children's Hospital, Boston.
DR. FISHMAN is Instructor in Surgery, Children's Hospital, Boston.
DR. LEICHTNER is Clinical Director, Division of Pediatric Gastroenterology and Nutrition, Children's Hospital, Boston.
DR. TUNNESSEN, who serves as Section Editor for Pediatric Puzzler, is Senior Vice President, American Board of Pediatrics, Chapel Hill, NC,and a member of the Contemporary Pediatrics Editorial Board.
















