





Pediatric Puzzler: Swollen eyes
Pediatric Puzzler: Swollen eyes (Orbital pseudotumor)
PEDIATRIC PUZZLER
GEORGE K. SIBERRY, MD, MPH, SECTION EDITOR
One boy, two swollen eyes:
Don't lose him in your blind spot!
By Brendan P. Lucey, Jennifer Huffman, MD, and Catherine Parrish, MD
Late one afternoon, your office receives a call from the mother of one of your patients, a 5-year-old boy, reporting that she's concerned about swelling around both of his eyes. You know the child and his mother well: He has a history of asthma and chronic allergic rhinitis, and his only regular medications are albuterol by metered-dose inhaler and cetirizine hydrochloride (Zyrtec). She noticed the swelling around his left eye six days ago, after which it progressed to include the right eye, although the left eye remains more affected. She reports that he has had no recent trauma, including lacerations or abrasions; no fever, insect bites, or chills; and no prior episodes of facial swelling, sinusitis, or cellulitis. The boy wears corrective glasses, but has no history of ocular injury or surgery. Mom attributes the periorbital swelling to seasonal allergy, and requests a refill of the cetirizine.
Two days later, Mom calls again for advice because the swelling has failed to resolve. Her son's left eye is irritated and itchy, she reports. You prescribe olopatadine hydrochloride ophthalmic solution (Patanol) and schedule telephone follow-up for the next day.
Nothing encouraging to be seen
By the next afternoon, there is no improvement in the boy's eye. Concerned that his condition remains unchanged, you direct Mom to bring him to the office that day. On examination, the boy appears well and is not in respiratory distress. He is afebrile; vital signs are within normal limits. He complains of pain in his left eye on movement of the lateral gaze. You note moderate periorbital edema of the left upper and lower eyelids; minimal erythema of the left upper eyelid; but no discharge from the eye, palpable masses, fluctuance, tenderness, or crepitus in the periorbital region. Facial and corneal sensations are intact bilaterally. Cardiac, pulmonary, nasal, and abdominal examinations are unremarkable.
Certainly, the situation has turned more troubling and less routine. Your patient has failed initial treatment for an allergic cause of bilateral periorbital swelling, and the initial differential diagnosis includes several worrisome entities. Infectious causes, such as preseptal and orbital cellulitis; trauma; and infiltrative processes such as thyroid disease, sarcoidosis, and tumor need to be considered. Your thorough history and physical examination allow you to eliminate trauma, and an infiltrative process doesn't seem likely. Preseptal cellulitis seems the most likely cause, despite his lack of fever. On that presumption, you prescribe oral amoxicillin-clavulanate, 90 mg/kg/day, and send him home.
Not a sight for sore eyes
In the 24 hours that follow, however, findings on examination become worse. The boy continues to be afebrile, but he develops proptosis and pain on eye movement in all directions. At this point, orbital cellulitisa medical emergencymust be excluded before investigating other diagnoses, or treated if present; no doubt, the patient needs a more thorough evaluation than you can give him in the office, so you send him to the hospital's emergency department.
Differentiating preseptal cellulitisinfection of the superficial tissue layers anterior to the orbital septumand postseptal cellulitisinvolving the orbit and usually a complication of acute ethmoid and sphenoid sinusitiscan be difficult. Signs and symptoms characteristically associated with preseptal cellulitisfever, edema, tenderness, warmth of the lidcan also be seen in postseptal cellulitis. Postseptal cellulitis is distinguished by proptosis, chemosis, impaired vision, limited extraocular movements, decreased mobility of the globe, and pain on movement of the globe.1
An ophthalmology consult is requested in the ED. Intraocular pressure is 12 mm on the right and 14 mm on the left (normal, <20 mm). Slit-lamp examination is unremarkable. Dilated fundoscopic examination reveals disk elevation on the left compared to the right. The disk appears mildly edematous but is neither pale nor hyperemic. No disk hemorrhages are seen.
Laboratory studies are also obtained. The white blood cell count is 8.6 x 103/uL; hemoglobin, 10.3 g/dL; hematocrit, 31.3%; and platelet count, 593 x 103/uL. The differential count, urinalysis, and basic blood chemistry tests are all normal. Blood is drawn for culture.
Clearly, the child has features of both preseptal and postseptal cellulitisproptosis, pain on eye movement, periorbital edema. But the absence of fever, chemosis, and tenderness also makes the presentation unusual for these infectious causes.
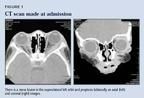
What's indicated now is imaging to distinguish between the processes that remain in your differential, particularly an infiltrative one. The initial ED reading of a maxillofacial computed tomographic (CT) scan without contrast demonstrates moderate-to-marked soft-tissue swelling in the preseptal tissues of the left eye, with extension into postseptal tissues (Figure 1).


After admission for assessment and treatment, your patient is placed on IV ceftriaxone and clindamycin (eventually completing a 10-day course). Blood cultures remain negative throughout his stay. He has a moderately positive response to the antibiotics over the first 72 hours, with diminished swelling in the left orbit, but the marked pain on eye movement and proptosis remain.
Two days later, you see the report of the official reading of the initial CT scan: there is abnormal soft-tissue density involving the superolateral left orbit, lacrimal gland, and superior and lateral rectus muscles (Figure 1). Sinuses and cranial nerves are unremarkable. Imaging findings are consistent with both inflammation or inflammatory tissue and with neoplasm. Consequently, you shift your focus to noninfectious processes in your differential diagnosis: rhabdomyosarcoma and lymphoid tumor secondary to leukemia or lymphoma.
Rhabdomyosarcoma is the most common primary orbital cancer of children, accounting for 9% of orbital masses in this population.1 The lesion usually presents as a mass that may or may not be painful. Symptoms are caused by displacement or obstruction of normal structures. Primary orbital rhabdomyosarcoma is diagnosed early in its course because of associated proptosis, periorbital edema, ptosis, a change in visual acuity, and local pain.1 In contrast, a lymphoid tumor of the orbit is rare in children. When it involves the orbit, this mass presents more insidiously and is usually painless. A lymphoid tumor tends to form a unifocal mass in the orbit that molds to surrounding structures.2
One week into his hospital stay, a repeat CT scan shows continued involvement of the left lateral and superior rectus extraocular muscles and of the left lacrimal gland. On hospital day 7, the ophthalmology service orders a biopsy of the left lacrimal gland, which shows a small population of lymphocytes, almost all of which are normal T cells. No findings of malignancy can be detected. The tentative diagnosis? Orbital pseudotumor. The boy's postoperative course is unremarkable.
"Here's a lesion in yer eye"
Orbital pseudotumor is defined as a nongranulomatous inflammatory process in the orbit or eye without a known local or systemic cause.3 The diagnosis should be entertained only after true neoplasm, primary infection, and other defined, often systemic, inflammatory diseases have been excluded. Pediatric orbital pseudotumors constitute 6% to 16% of all orbital pseudotumors.3 The condition is uncommon in children. When the adult and pediatric pseudotumor populations are compared, bilateral orbital involvement emerges as nearly the rule, not the exception, among children; bilateral orbital involvement in adults, on the other hand, strongly suggests systemic disease.2
Although the diagnosis of orbital pseudotumor is one of exclusion, certain features of the history and physical exam are useful in making decisions. Swelling (in 93% of cases), pain (in 69%), ptosis (42%), headache (38%), and photophobia (28%) are most common.2 Vomiting, diplopia, erythema, pain on eye movement, and sore throat are less common. Constitutional symptomsfever, malaiseare common in children with inflammatory pseudotumor. On examination, common signs include proptosis (in 80% of cases), a motility defect (in 70%), and injection (55%).2 Less common are a palpable mass, ptosis, uveitis, iritis, tenderness, retinal striae, and erythema.
The presentation of pseudotumor, rhabdomyosarcoma, and lymphoid tumor in the orbit also differ markedly from each other. Pseudotumor is, first, a more acute process than rhabdomyosarcoma or a lymphoid tumor and, second, forms irregularly shaped, apparently infiltrative, mass lesions, particularly at distinctive anatomic locations, including Tenon's space, perioptic nerve connective tissues, lacrimal glands, and extraocular muscles.2 Fibrosis of these structures leads to greater morbidity, such as motility restriction and optic nerve compression.
Laboratory studies are not very helpful in differentiating pseudotumor from cellulitis. That being said, with pseudotumor one will unvaryingly see an elevated erythrocyte sedimentation rate and, in 30% of cases, an eosinophilia on the peripheral smear. By the nature of the process, blood cultures taken from a patient with pseudotumor are negative. A CT scan of the orbits and sinuses made with fine cuts will delineate the extent of any mass and demonstrate possible sinusitis. The presence of normal sinuses on CT (as in this patient) is highly uncommon in orbital cellulitis. Sinusitis does not support a diagnosis of orbital cellulitis to the exclusion of pseudotumor, however.2
Once orbital cellulitis has been ruled out, a trial of steroids may be attempted. A response would be indicative of pseudotumor; no further work-up is then necessary. Biopsy (open preferred over fine needle aspiration) should be attempted in patients who are unresponsive to antibiotics or steroids. Given the prevalence of rhabdomyosarcoma in the pediatric population, however, proceeding straight to biopsy might be preferable.
Based on the clinical presentation and findings on both the CT scan and biopsy, orbital pseudotumor is the suspected cause of this child's signs and symptoms. He is treated with oral prednisone, 2 mg/kg/day. You witness improvement before he is discharged, in the form of diminished orbital swelling and proptosis. He is sent home with a prescription for oral prednisone and an appointment for follow-up with you one week later.
At follow-up, the boy denies pain; periorbital swelling is improving, although slowly. Because resolution is slow, you order thyroid function studies, which return normal, to rule out thyroid orbitopathy, and a chest radiograph, which is negative, to rule out sarcoidosis. He continues on prednisone with a slow taper. A follow-up CT scan is normal (Figure 2). The boy continues to improve clinically. And you set your sights on another diagnostic challenge. Here's looking at you!



REFERENCES
1. Traboulsi EI, Maumentee IH: Eye problems: Tumors, in McMillan JA, DeAngelis CD, Feigin RD, et al: Oski's Pediatrics: Principles and Practice, ed 3. Baltimore, Md., Lippincott Williams &Wilkins, 1999: pp 675677
2. Berger JW, Rubin PAD, Jakobiec FA: Pediatric orbital pseudotumor: Case report and review of the literature. Int Ophthalmol Clin 1996;36:161
3. Weber AL, Romo LV, Sabates NR: Pseudotumor of the orbit. Clinical, pathologic, and radiologic evaluation. Radiol Clin North Am 1999;37:151
MR. LUCEY is a medical student at The Johns Hopkins University School of Medicine, Baltimore, Md.
DR. HUFFMAN is a resident in the department of pediatrics, The Johns Hopkins Hospital.
DR. PARRISH is in pediatric practice at Tindeco Health Center, Baltimore, and is a part-time member of the faculty of the department of pediatrics at The Johns Hopkins University School of Medicine.
DR. SIBERRY is an assistant professor of pediatrics in the divisions of general pediatric and adolescent medicine and pediatric infectious diseases at The Johns Hopkins Hospital.
Brendan Lucey, Catherine Parrish, Jennifer Huffman. Pediatric Puzzler: Swollen eyes.
Contemporary Pediatrics
August 2003;20:25.





Having "the talk" with teen patients
June 17th 2022A visit with a pediatric clinician is an ideal time to ensure that a teenager knows the correct information, has the opportunity to make certain contraceptive choices, and instill the knowledge that the pediatric office is a safe place to come for help.


Artificial intelligence improves congenital heart defect detection on prenatal ultrasounds
January 31st 2025AI-assisted software improves clinicians' detection of congenital heart defects in prenatal ultrasounds, enhancing accuracy, confidence, and speed, according to a study presented at SMFM's Annual Pregnancy Meeting.



