





Ranulas in a 14-Year-Old Boy
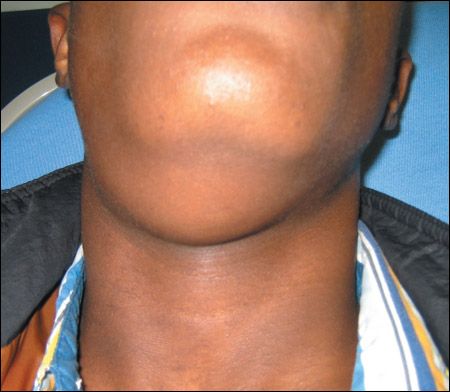
14-Year-old boy who presents to emergency department with nonpainful swelling under his chin that began about a week earlier. Swelling has been gradually growing; patient now has some difficulty in flexing his neck.


HISTORY
14-Year-old boy who presents to emergency department with nonpainful swelling under his chin that began about a week earlier. Swelling has been gradually growing; patient now has some difficulty in flexing his neck.
Patient appears otherwise healthy and has no significant medical history. No recent fever or trauma. Vital signs, including blood pressure, normal.


PHYSICAL EXAMINATION
Large, soft, right-sided mass, palpable from the tip of chin down to the level of the cricoid cartilage. Not warm, red, or tender to palpation. No movement of the mass with swallowing; it does not cross the midline. Patient is not drooling and has no respiratory difficulty. Posterior oropharynx,soft palate, and dentition all normal. Patient can open his mouth without difficulty.
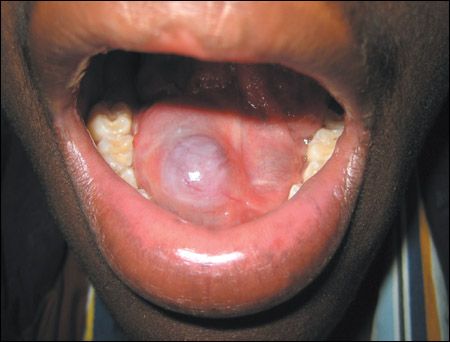
Examination of the underside of the tongue reveals a blue cystic mass on the floor of the mouth. This right-sided mass appears to be fluid-filled: no pus, blood, or debris apparent.
"WHAT'S YOUR DIAGNOSIS?"
ANSWER: RANULAS
Ranulas are pseudocysts that develop when mucus leaks into surrounding tissues. They arise from major salivary glands; mucoceles arise from minor salivary glands. Both mucoceles and ranulas may occur secondary to trauma or to blocked salivary excretion.
There are 2 types of ranulas: oral and plunging.
Usually painless, and frequently asymptomatic, oral ranulas can sometimes cause problems with oral function--including speech, swallowing, and occasionally, respiration. An oral ranula appears as a blue-hued translucent swelling on the floor of the mouth that resembles the belly of a frog.This rare fluid-filled mass is compressible and painless.
Rarer still is the plunging ranula.1 Usually seen coincidentally with an oral ranula (as with this patient), a plunging ranula can arise without the blue translucent swelling at the floor of the mouth.
Needle aspiration may be therapeutic; however, swelling generally recurs. Other methods of treatment include marsupialization as well as excision of the ranula and the offending sublingual gland.2 In one study, the recurrence rates with these methods were 66.67%, 57.69%, and 1.2%, respectively.3
This patient initially underwent marsupialization. The lesion recurred about 4 months later. Ultimately, the ranula was excised and the involved sublingual gland was obliterated. The patient is currently doing well.
References:
REFERENCES:
1.Langlois NE, Kolhe P. Plunging ranula: a case report and a literature review.
Hum Pathol.
1992;23:1306-1308.
2.Morita Y, Sato K, Kawana M, et al. Treatment of ranula--excision of the sublingual gland versus marsupialization.
Auris Nasus Larynx.
2003;30:311-314.
3.Zhao YF, Jia Y, Chen XM, Zhang WF. Clinical review of 580 ranulas.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
2004;98:281-287.
FOR MORE INFORMATION
Patel NJ, Sciubba J. Oral lesions in young children. Pediatr Clin North Am. 2003;50:469-486.
Schneiderman H, Nzeako UC. Ranula. Consultant. 1996;36:311-312.











Recognize & Refer: Hemangiomas in pediatrics
July 17th 2019Contemporary Pediatrics sits down exclusively with Sheila Fallon Friedlander, MD, a professor dermatology and pediatrics, to discuss the one key condition for which she believes community pediatricians should be especially aware-hemangiomas.





