





Case In Point: Eczema Herpeticum: An Uncommon Complication of Atopic Dermatitis
A 2-year-old boy was brought for evaluation of a rash and fever of 2 days' duration. He had atopic dermatitis since 6 months of age that was partially controlled with low-potency topical corticosteroids and emollients. His father reported that recently the facial dermatitis had worsened, with increased redness, pain, and some skin breakdown. The child's medical history was otherwise unremarkable. His mother had a history of "cold sores."
A 2-year-old boy was brought for evaluation of a rash and fever of 2 days' duration. He had atopic dermatitis since 6 months of age that was partially controlled with low-potency topical corticosteroids and emollients. His father reported that recently the facial dermatitis had worsened, with increased redness, pain, and some skin breakdown. The child's medical history was otherwise unremarkable. His mother had a history of ;cold sores.;
The patient was irritable during the examination; temperature was 40°C (104°F).He had scaly, erythematous patches on the extensor surfaces of all extremities. Lichenified plaques were present on the wrists and ankles. There were multiple monomorphic, 3- to 4-mm, umbilicated, crusted vesicopustules with erythema on the face, particularly on the forehead above the right eye (Figure 1).



Figure 1

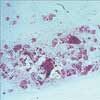
Figure 2
No conjunctiva involvement or ocular symptoms were noted.
The history and clinical features are typical of eczema herpeticum. A Tzanck smear of a specimen taken from the base of involved vesicles revealed multinucleated giant cells, con- sistent with herpesvirus (Figure 2).
The patient was treated with oral acyclovir, 400 mg tid for 7 days. In addition, cephalexin, 250 mg tid for 7 days, was given because of a suspected secondary Staphylococcus aureus infection, indicated by the yellow crusting. At follow-up, the lesions and fever had resolved.
ECZEMA HERPETICUM: CAUSE AND PREVALENCE
Atopic dermatitis, which affects between 12% and 26% of children in the United States, has become increasingly common over the past 30 years.1 Superimposed viral infection is an uncommon complication of atopic dermatitis. Atopic patients are prone to opportunistic infection because their skin barrier is compromised and their immune response may be suppressed.
Kaposi varicelliform eruption refers to a cutaneous herpes simplex virus (HSV) infection in patients with a preexisting dermatosis.1 Eczema herpeticum represents HSV infection in the setting of atopic dermatitis.2 Eczema herpeticum can be caused by either type 1 or type 2 HSV.
Epidemiologic data on eczema herpeticum are scarce; however, there has been an increase in the number of patients treated for the condition in university hospitals in recent years.3 Eczema herpeticum may be associated with an early onset of atopic dermatitis and a high total serum IgE level.2
CLINICAL FEATURES
Atopic dermatitis typically manifests as poorly defined, erythematous, scaling patches on the extensor surfaces of the extremities (Figure 3).



Figure 3Eczema herpeticum appears superimposed on these surfaces and may spread to normal skin. Patients have monomorphic eruptions of dome-shaped vesicles, which may transform into pustules. The vesicles dry out within 2 to 3 weeks and may leave erosive pits. These ;punched out; erosions can create a scalloped appearance at the periphery of the large denuded area.
4
Patients often contract the virus by direct contact with an infected person (eg, a kiss from a parent with herpes labialis).5 Eczema herpeticum can also occur in the setting of a primary HSV infection.
Complications are rare. Secondary bacterial infection with S aureus or b-hemolytic streptococci may occur. High fever and other systemic symptoms herald this possibility.2 In addition, periorbital eczema herpeticum can result in keratoconjunctivitis with possible stromal scarring and subsequent blindness. Refer patients who have eye involvement for immediate ophthalmologic evaluation.
DIAGNOSIS
In persons with atopic dermatitis, eczema herpeticum may be suspected based on the appearance of the vesicular lesions and the accompanying symptoms (ie, fever, lymphadenopathy, and malaise). The lesions are usually very painful. This frequently distinguishes them from other dermatoses--such as widespread impetigo, molluscum contagiosum, and blistering disorders of childhood. Often, eczema herpeticum is assumed to be an exacerbation of the primary atopic dermatitis.
The diagnosis can be easily suggested by a Tzanck smear--performed by unroofing a vesicle and scraping the base of a lesion. On light microscopic examination, typical findings of viral infection include acantholytic balloon cells with multinucleated giant cells. HSV infection can be confirmed by culture of a swab of the lesions or by a direct fluorescent antibody test. When a secondary infection is suspected, obtain a bacterial culture.2
TREATMENT
Eczema herpeticum is usually managed on an outpatient basis. Inpatient treatment is reserved for patients with more severe cases (eg, high fever, poor oral intake, evidence of secondary infection). Acyclovir remains the most studied and frequently used treatment. The pyrophosphate analog foscarnet is also effective and may be used in the rare case of acyclovir-resistant herpes.1
When eczema herpeticum involves the skin around the eye, a topical ophthalmic antiviral may be added for keratitis prophylaxis. For the treatment of bacterial superinfection, an oral cephalosporin and topical antiseptic lotion may be adequate. Treatment with topical or systemic corticosteroids is still controversial: most clinicians avoid it.2
PROGNOSIS
Before the availability of effective antiviral treatment, mortality associated with eczema herpeticum was as high as 75%.2 Mortality is now very low. Although the average duration of illness is 16 days,1 cases lasting as long as 6 weeks have been reported. Recurrent episodes tend to be milder and are not associated with systemic symptoms.
References:
REFERENCES:
1.
Mooney MA, Janniger CK, Schwartz RA. Kaposi's varicelliform eruption.
Cutis.
1994;53:243-245.
2.
Wollenberg A, Wetzel S, Burgdorf WH, Haas J. Viral infections in atopic dermatitis: pathogenic aspects and clinical management.
J Allergy Clin Immunol.
2003;112:667-674.
3
. Wollenberg A, Zoch C, Wetzel S, et al. Predispoing factors and clinical features of eczema herpeti-cum: a retrospective analysis of 100 cases.
J Am
Acad Dermatol.
2003;49:198-205.
4.
Katta R. Painful skin erosions and fever in an infant. Eczema herpeticum.
Postgrad Med.
2001;109: 129-130.
5.
Mackley CL, Adams DR, Anderson B, Miller JJ. Eczema herpeticum: a dermatologic emergency.
Dermatol Nurs.
2002;14:307-310.








Recognize & Refer: Hemangiomas in pediatrics
July 17th 2019Contemporary Pediatrics sits down exclusively with Sheila Fallon Friedlander, MD, a professor dermatology and pediatrics, to discuss the one key condition for which she believes community pediatricians should be especially aware-hemangiomas.





