





Differentiating Epileptic Seizures From Nonepileptic Spells
It can be difficult to determine whether unusual, paroxysmal behavior represents a seizure or a nonepileptic event. Children with sudden flailing movements or unresponsive staring may, in fact, be experiencing psychogenic events.
It can be difficult to determine whether unusual, paroxysmal behavior represents a seizure or a nonepileptic event. Children with sudden flailing movements or unresponsive staring may, in fact, be experiencing psychogenic events. Other types of pathological spells, such as syncope and migraine, can also be mistaken for epileptic seizures. When epilepsy is incorrectly diagnosed in these patients, unnecessary seizure medication is likely to be prescribed, and correct diagnosis and treatment is delayed. It is also the case that epileptic seizures can be subtle and difficult to recognize. Inattentive staring may be attributed to attention deficit disorder but may, in fact, be due to either absence or complex partial seizures.
An orderly approach to the differential diagnosis of paroxysmal events is the best way to avoid misdiagnosis. A careful, detailed history and physical examination supplemented by an electroencephalogram (EEG) will, in most cases, result in a correct diagnosis.
EPILEPTIC SEIZURES
Epileptic seizures are paroxysmal, abnormal behaviors caused by excessive, hypersynchronous firing of neurons in the brain. Most seizures arise in the cerebral cortex, although subcortical structures can also generate seizures.1,2 The incidence of epilepsy is highest in early childhood and peaks again late in life.3 When epilepsy is attributed to a brain abnormality (eg, mental retardation, cerebral palsy, malformation), it is classified as "symptomatic." Epilepsy is considered "idiopathic" when there is no recognized brain abnormality.4
MORBIDITY
The risk of recurrence within 2 years after a first-time, unprovoked seizure is approximately 35% to 40%.5 Increased risk of recurrence is associated with factors such as a remote, symptomatic cause (eg, brain injury); abnormal EEG; and seizure during sleep. Treatment with antiepileptic medication reduces the risk of a recurrence after a first seizure, but there is little evidence that treatment prevents the later development of epilepsy.6
Prolonged seizures can cause brain injury, but epidemiological studies have not provided evidence that prolonged first seizures in otherwise healthy persons increase the risk of subsequent seizures.7 Furthermore, the number of seizures that occur before treatment is initiated is not necessarily associated with a greater likelihood of medical intractability. 8 Seizure frequency and whether the seizures are generalized or partial have stronger predictive power. Therefore, little advantage is gained by treating first-time seizures, whether they are provoked by an identified acute insult or they occur out of the blue. The rationale for treating children with recurrent seizures is that treatment will ameliorate seizure recurrence.
DIAGNOSTIC SUSPICION
Most often, seizure history related by the patient's parents and the physical findings will lead the physician to suspect epilepsy. For example,a history of febrile seizures (particularly if prolonged) is a well-recognized risk factor for the development of temporal lobe epilepsy caused by mesial temporal sclerosis.9,10 An additional helpful clue from the history is a past brain injury from trauma or infection. It is generally understood that relatively remote trauma of a minor degree confers very little risk, but prolonged loss of consciousness or a penetrating head injury are significant risk factors for seizure episodes. 11,12 A family history is important, because epilepsy in first-degree relatives is another risk factor.
Physical examination findings that indicate an abnormality of brain function provide further evidence of an increased likelihood of seizures. They also help classify epilepsy as either symptomatic or idiopathic. For example, mental retardation, cerebral palsy, or the presence of neurocutaneous lesions is noteworthy. Cerebral imaging studies may demonstrate a structural brain abnormality.
Certain circumstances can erroneously heighten suspicion of seizures by the patient, parent, and physician. Benign or at least nonepileptic behaviors may be mistakenly identified as seizures or described in rather dramatic terms. Table 1 provides a brief overview of nonepileptic events that mimic specific seizure types that occur particularly in children.


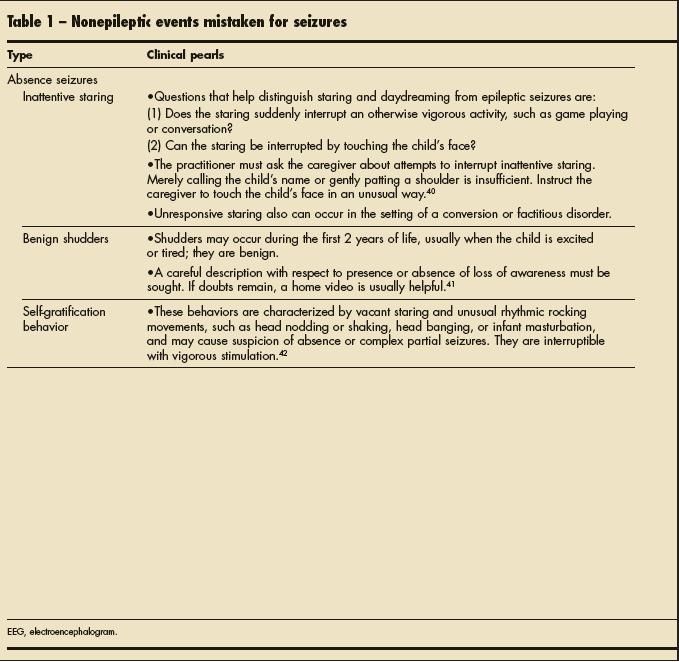
Table 1
Parents of children who have health challenges that may include previous seizures may be very sensitive to any perceived abnormality in the child's health. Benign events, such as hypnic jerks, may prove very frightening to the parents of a child who recently suffered a febrile seizure. A child with autism may have stereotyped movements that convince a concerned parent that the child is having seizures. Munchausen syndrome and Munchausen syndrome by proxy also may present as seizures.13,14 When the history suggests seizure, a careful differential diagnosis is important.
NONEPILEPTIC EVENTS
Nonepileptic seizures are behavioral events that resemble epileptic seizures but are not caused by abnormal, hypersynchronous neuronal discharges in the brain. The term "pseudoseizure" is discouraged, since the events themselves are real and disabling. Nonepileptic events can be caused by psychological disorders, or they can be manifestations of other pathological or physiological neurological conditions.
Alternating hemiplegia. This is characterized by repeated bouts of dystonic posturing accompanied by nystagmus. Hemiplegia can occur on either side or bilaterally. It occurs in the presence of developmental regression and persistent developmental delay. Onset is usually during infancy. The condition has been variously attributed to a migrainous mechanism, epilepsy, and movement disorder. The underlying cause has been linked to mitochondrial dysfunction, channelopathies, and small vessel disease. The calcium channel blocker flunarizine has been used in treatment, as has topiramate.15,16
Benign sleep movements. Benign myoclonus or hypnic jerks often occur shortly after falling asleep. Movements during rapid eye movement sleep also may be mistaken for seizures. Correct identification of these events often will allay the parents' anxiety. However, if a child has experienced a seizure (eg, a febrile convulsion) previously, parents may be hypervigilant. Asking the parents to record a video of such movements may be helpful.17
Breath-holding spells (BHS). These spells commonly begin between the ages of 6 and 18 months. They are characterized by hard crying in response to injury or anger and breath-holding, stiffening, and cyanosis (or sometimes pallor) followed by brief loss of muscle tone and consciousness.
Pallid BHS are a type of syncope. They are more likely to occur in reaction to an event causing injury, pain, or emotional distress.18,19 Some children hold their breath on inspiration before getting the first cry out. Others hold their breath in expiration. They usually stop the behavior by age 5 or 6 years. A family history of BHS is common.
BHS are generally benign but can occasionally provoke acute reactive seizures, presumably caused by transient cerebral hypoxia in much the same way syncope can provoke acute seizures. Recognition depends on taking a careful history that looks for consistent initial crying and cyanosis or pallor early in the attack. Treatment for routine BHS consists of reassurance. Some evidence suggests that iron supplementation helps some children.20.
Gastroesophageal reflux. Symptoms associated with gastroesophageal reflux may be mistaken for seizures. Infants may have stiffening and crying episodes suggestive of infantile spasms. Older children, particularly if they are cognitively impaired and not able to communicate well, may have reflux-related pain leading to stiffening episodes that are reminiscent of tonic seizures, or they may have sudden behavior changes suggesting partial seizures. Abnormal posturing in children with gastroesophageal reflux is often referred to as Sandifer syndrome.21,22
Syncope. The distinction between epileptic seizures and syncope can be particularly challenging. Transient loss of consciousness-particularly if accompanied by body stiffening- can suggest seizures, but positive motor signs are common in syncope. At the same time, transient cerebral hypoperfusion occurring during syncope can cause an acute reactive seizure (convulsive syncope).
Features suggesting syncope include preceding light-headedness, sweating, pallor, prolonged standing, sudden changes in posture-from lying down to sitting or standing- and precipitation by vagal stimuli, such as micturition. Conversely, typical aura (eg, epigastric rising sensation, dj vu), postictal delirium, and focal physical features, such as head turning, are suggestive of seizure.23 An EEG showing epileptiform discharges or postictal slowing can help confirm the diagnosis. An ECG revealing an arrhythmia or a positive tilt table test suggests syncope.24
There are also rare cases in which a seizure provokes asystole. When such cases are recognized, the insertion of a pacemaker is often recommended.25
Conversion disorder. Conversion disorders can manifest as psychogenic nonepileptic seizures (PNES). A history of significant social stresses should alert a clinician to the possibility of PNES. Some apparent secondary gain usually will be associated with the spells, although in conversion disorder, the patient is not consciously producing the symptom. Such gains may include being sent home from school or averting physical abuse.
A history of physical or sexual abuse should be considered when PNES are diagnosed. Less severe stresses such as high academic pressure or bullying at school also may cause symptoms.
A number of physical features during seizure episodes are suggestive of PNES. The eyes are usually closed.26 Asynchronous clonic limb movements (flailing) are often present. Other symptoms include pelvic thrusting and prominent rotatory (horizontal back and forth) head movements. An unusual lack of concern about the symptoms (la belle indifference affect) is typical. Also, it is unusual for persons with PNES to have the seizures during sleep. Incontinence and self-injury also are less common during PNES than in epileptic seizures.27
The above-noted symptoms are suggestive but not definitive. It is important to document the nonepileptic nature of these disabling events; video EEG monitoring is most trusted. It may be challenging to get the suspicious event to occur in the clinical setting. Various forms of suggestion have been used to trigger events, but ethical considerations need to be acknowledged. Hypnosis also has been successfully used to provoke PNES in children.28,29
It is never adequate to simply give a diagnosis of PNES without further treatment. The episodes remain disabling despite reassurance that the spells are not epilepsy. If the underlying stresses contributing to the spells go untreated, and if adequate coping mechanisms are not adopted, it is likely that the spells will continue. Referral to a child psychologist or psychiatrist is necessary. Early diagnosis of PNES carries a better prognosis for remission.30
EPILEPTIC SEIZURE TYPES
Generalized motor seizures. The types of generalized motor seizures (Table 2) are relatively easy to diagnose based on patient history. However, there are physiological and psychogenic behaviors that can be mistaken for these relatively dramatic epileptic seizures. Nonepileptic events that suggest generalized motor seizures include chorea, athetosis, dystonia, and opisthotonus. Because such behaviors are frequently (but not exclusively) encountered in developmentally disabled children, a history of normally maintained consciousness and awareness may be difficult to ascertain.

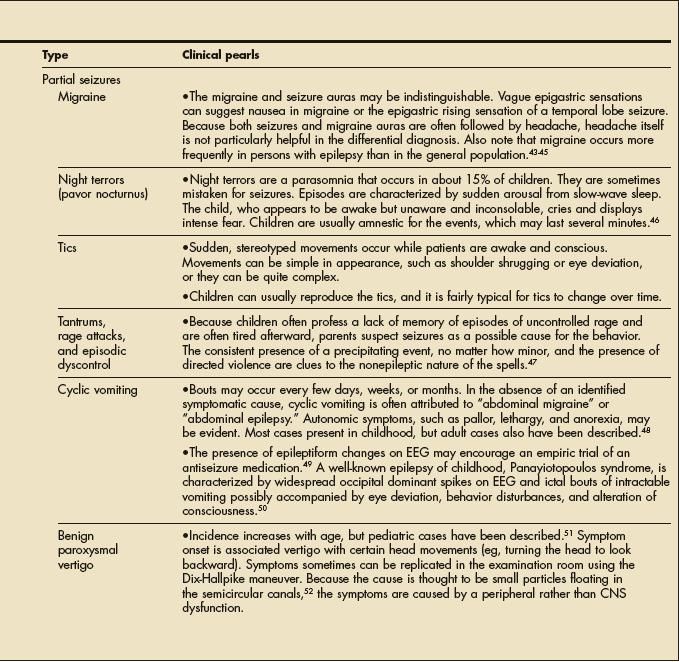
Table 2
More complex movements, such as chorea or athetosis, are characterized by writhing or jerking. They are usually distinguishable from seizures because of the absence of a clear rhythmic component (unlike clonic seizures). The movements are often bilateral and awareness is maintained. Because the movements may be generalized or focal, they may be mistaken for either generalized or partial seizures.31
Absence seizures. These seizures are characterized by discrete episodes of unresponsive staring and are sometimes accompanied by minor automatisms such as eye blinking or head titubation. In the untreated person, they usually occur many times a day. Each episode may last from a few to about 30 seconds. The frequency of the seizures, their short duration, and the relative absence of automatisms help distinguish absence seizures from complex partial seizures.
Behavioral nonepileptic events such as inattention or daydreaming may be hard to distinguish from absence seizures unless there is a clear history of a lack of response to physical stimulation. An EEG is helpful, because untreated persons with absence epilepsy will almost always have generalized spike wave discharges. Atypical absence seizures are usually longer and have more accompanying subtle motor symptoms. They are commonly seen in cognitively impaired children who have other, more obvious seizure types. Lennox-Gastaut syndrome is a common setting for atypical absence seizures.32
Partial seizures. These seizures present the greatest diagnostic challenge because of the many symptoms that can be manifestations of epileptic activity. Loss of awareness is a clinical feature that distinguishes complex from simple partial seizures. A wide variety of automatisms can be present during partial seizures depending on the part of the brain involved. Seizures arising from the frontal convexity or parasagittal region often are associated with prominent motor signs. Subtler motor activity that may be mistaken for absence seizures is indicative of orbital frontal and frontopolar seizures. Typical temporal lobe symptoms may include dizziness, staring, autonomic changes, and subtler, semipurposeful automatisms such as picking at clothes and chewing. Parietal and occipital onset is suggested by initial sensory and visual symptoms, respectively.
SUBTLE OR SUBCLINICAL SEIZURES
There are some circumstances in which seizure manifestations may be quite subtle and may show up only on an EEG. Patients in an unexplained coma or with waxing and waning levels of consciousness may be experiencing subtle seizures or nonconvulsive status epilepticus. An unexplained acute encephalopathy, particularly in the setting of a brain insult, should raise the possibility of seizure and prompt an EEG evaluation.
Other conditions in which subtle or subclinical seizures should be suspected as part of the differential diagnosis are Landau-Kleffner syndrome (LKS) and continuous spike and waves during slow sleep (CSWS).
Landau-Kleffner syndrome. LKS affects children and its hallmark is aphasia in the setting of relatively mild epilepsy. To make this diagnosis, the child must demonstrate loss of language skills and have either a history of seizures or an EEG showing epileptiform abnormalities. Some 20% of affected children have epileptiform EEG abnormalities without a history of clinical seizures. No specific EEG pattern is pathognomonic, but temporal maximum spikes often are described. Treatment is aimed at reducing the frequency of interictal spike discharges using such medications as valproate, benzodiazepines, and corticosteroids. Multiple subpial transection also has been used for treatment of medically refractory cases.33,34
Continuous spike and waves during slow sleep. CSWS, also known as electrical status epilepticus during slow-wave sleep, is a condition in which nearly continuous (more than 85%) spike-wave discharges are seen on the EEG during deep slow-wave sleep. Age at onset is usually 2 to 9 years, and the phenomenon is associated with language, cognitive, and behavioral impairments. Although most affected children have a history of seizures (either generalized or partial), cases identified only through EEG findings have been described. The cause may be cryptogenic or symptomatic.35
THE ROLE OF EEG
A routine EEG performed in a child with a presumed first seizure will show epileptiform abnormalities about 7% to 34% of the time. An EEG performed in the first 24 hours after an attack increases the EEG yield to 51%.36 Repeated EEGs, sleep deprivation before the EEG, and sleep recorded during the EEG all increase the likelihood of recording epileptiform discharges.37 Nevertheless, some children with epilepsy will persistently have normal EEGs, and some children with epileptiform spike discharges may have a statistically increased risk but never experience a seizure.
Ideally, a seizure event should be captured on EEG, but this is seldom practical in the outpatient laboratory. If the events are reasonably frequent, a long-term EEG that records the habitual attacks helps provide diagnostic certainty.38 Both inpatient and outpatient long-term EEG are feasible, and outpatient video recording during EEG is increasingly practical, but the inpatient setting provides much more control over video recording conditions.
For seizures with altered consciousness, the EEG will almost always show some paroxysmal change, and most of the time an evolving rhythmic ictal discharge will be apparent if the seizures are epileptic. Exceptions include some frontal lobe seizures in which the epileptogenic cortex is distant from recording scalp electrodes, such as in the mesial frontal or the orbital frontal region. Even in such cases, a paroxysmal EEG change, such as slowing, will be evident, but prominent movement artifacts may obscure the EEG. Other exceptions include auras or simple partial seizures. Not enough of the cortex may be synchronized to allow recording of the rhythmic discharges from the scalp electrodes.39
Because it is important that children who are hospitalized for video EEG recordings have their habitual seizures, antiepileptic drugs often are tapered. For patients with mixed epileptic and nonepileptic events, drug tapering presents a problem because drug withdrawal may simply uncover the epileptic attacks that were pharmacologically controlled, although the patient may also experience nonepileptic spells. It is important to document the variety of attacks in question and make sure that the video EEG captures the habitual events and not anomalous seizures that are provoked solely by medication withdrawal.
CLINICAL HIGHLIGHTS
- The distinction between epileptic seizures and syncope can be particularly challenging. Transient loss of consciousness-particularly if accompanied by body stiffening-can suggest seizures, but positive motor signs are common in syncope.
- Conversion disorders can manifest as psychogenic nonepileptic seizures (PNES) in adults and children. A history of significant social stresses points to the possibility of PNES.
- Behavioral nonepileptic events such as inattention or daydreaming may be hard to distinguish from absence seizures unless there is a clear history of a lack of response to physical stimulation. An electroencephalogram (EEG) is helpful, because untreated persons with absence epilepsy will almost always have generalized spike wave discharges.
- An EEG performed in the first 24 hours after a presumed seizure will show epileptiform abnormalities 51% of the time. Repeated EEGs, sleep deprivation before the EEG, and sleep recorded during the EEG all increase the likelihood of recording epileptiform discharges.
References:
1.
Kerrigan JF, Ng YT, Chung S, Rekate HL. The hypothalamic hamartoma: a model of subcortical epileptogenesis and encephalopathy.
Semin Pediatr Neurol.
2005;12:119-131.
2.
Norden AD, Blumenfeld H. The role of subcortical structures in human epilepsy.
Epilepsy Behav.
2002;3:219-231.
3.
Hauser WA, Annegers JF, Rocca WA. Descriptive epidemiology of epilepsy: contributions of population- based studies from Rochester, Minnesota.
Mayo Clin Proc.
1996;71:576-586.
4.
ILAE classification of epilepsies: its applicability and practical value of different diagnostic categories. Osservatorio Regionale per L’Epilessia (OREp), Lombardy.
Epilepsia.
1996;37:1051-1059.
5.
Berg AT, Shinnar S. The risk of seizure recurrence following a first unprovoked seizure: a quantitative review.
Neurology.
1991;41:965-972.
6.
Holmes GL, Zhao Q. Choosing the correct antiepileptic drugs: from animal studies to the clinic.
Pediatr Neurol.
2008;38:151-162.
7.
Shinnar S, Berg AT, Moshe SL, Shinnar R. How long do new-onset seizures in children last?
Ann Neurol.
2001;49:659-664.
8.
Camfield C, Camfield P, Gordon K, Dooley J. Does the number of seizures before treatment influence ease of control or remission of childhood epilepsy? Not if the number is 10 or less.
Neurology.
1996;46:41-44.
9.
Provenzale JM, Barboriak DP, VanLandingham K, et al. Hippocampal MRI signal hyperintensity after febrile status epilepticus is predictive of subsequent mesial temporal sclerosis.
AJR.
2008;190:976-983.
10.
Bender RA, Baram TZ. Epileptogenesis in the developing brain: what can we learn from animal models?
Epilepsia.
2007;48(suppl 5):2-6.
11.
De Santis A, Sganzerla E, Spagnoli D, et al. Risk factors for late posttraumatic epilepsy.
Acta Neurochir Suppl (Wien).
1992;55:64-67.
12.
Willmore LJ. Posttraumatic epilepsy.
Neurol Clin.
1992;10:869-878.
13.
Moldavsky M, Stein D. Munchausen syndrome by proxy: two case reports and an update of the literature.
Int J Psychiatry Med.
2003;33:411-423.
14.
Willis T, Roper H, Rabb L. Lamotrigine poisoning presenting as seizures: a case of deliberate poisoning.
Child Abuse Negl.
2007;31:85-88.
15.
Di Rosa G, Spanò M, Pustorino G, et al. Alternating hemiplegia of childhood successfully treated with topiramate: 18 months of follow-up.
Neurology.
2006;66:146.
16.
Neville BG, Ninan M. The treatment and management of alternating hemiplegia of childhood.
Dev Med Child Neurol.
2007;49:777-780.
17.
Di Capua M, Fusco L, Ricci S, Vigevano F. Benign neonatal sleep myoclonus: clinical features and video-polygraphic recordings.
Mov Disord.
1993;8:191-194.
18.
Goraya JS, Virdi VS. Persistence of breathholding spells into late childhood.
J Child Neurol.
2001;16:697-698.
19.
Lombroso CT, Lerman P. Breathholding spells (cyanotic and pallid infantile syncope).
Pediatrics.
1967;39:563-581.
20.
Daoud AS, Batieha A, al-Sheyyab M, et al. Effectiveness of iron therapy on breath-holding spells.
J Pediatr.
1997;130:547-550.
21.
Nanayakkara CS, Paton JY. Sandifer syndrome: an overlooked diagnosis?
Dev Med Child Neurol.
1985;27:816-819.
22.
Somjit S, Lee Y, Berkovic SF, Harvey AS. Sandifer syndrome misdiagnosed as refractory partial seizures in an adult.
Epileptic Disord.
2004;6:49-50.
23.
Benton TJ, Narayanan D. Differentiating seizure and convulsive syncope: the importance of history taking.
Postgrad Med.
2008;120:50-53.
24.
McKeon A, Vaughan C, Delanty N. Seizure versus syncope.
Lancet Neurol.
2006;5:171-180.
25.
Strzelczyk A, Bauer S, Knake S, et al. Ictal asystole in temporal lobe epilepsy before and after pacemaker implantation.
Epileptic Disord.
2008;10:39-44.
26.
Chung SS, Gerber P, Kirlin KA. Ictal eye closure is a reliable indicator for psychogenic nonepileptic seizures.
Neurology.
2006;66:1730-1731.
27.
Peguero E, Abou-Khalil B, Fakhoury T, Mathews G. Self-injury and incontinence in psychogenic seizures.
Epilepsia.
1995;36:586-591.
28.
Olson DM, Howard N, Shaw RJ. Hypnosisprovoked nonepileptic events in children.
Epilepsy Behav.
2008;12:456-459.
29.
Barry JJ, Atzman O, Morrell MJ. Discriminating between epileptic and nonepileptic events: the utility of hypnotic seizure induction.
Epilepsia.
2000;41:81-84.
30.
Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness.
Epilepsia.
2000;41:1330-1334.
31.
Lüders HO. Paroxysmal choreoathetosis.
Eur Neurol.
1996;36(suppl 1):20-23.
32.
Goldsmith IL, Zupanc ML, Buchhalter JR. Long-term seizure outcome in 74 patients with Lennox-Gastaut syndrome: effects of incorporating MRI head imaging in defining the cryptogenic sub-- group.
Epilepsia.
2000;41:395-399.
33.
Castillo EM, Butler IJ, Baumgartner JE, et al. When epilepsy interferes with word comprehension: findings in Landau-Kleffner syndrome.
J Child Neurol.
2008;23:97-101.
34.
Trevathan E. Seizures and epilepsy among children with language regression and autistic spectrum disorders.
J Child Neurol.
2004;19(suppl 1):S49-S57.
35.
Nickels K, Wirrell E. Electrical status epilepticus in sleep.
Semin Pediatr Neurol.
2008;15:50-60.
36.
King MA, Newton MR, Jackson GD, et al. Epileptology of the first-seizure presentation: a clinical, electroencephalographic, and magnetic resonance imaging study of 300 consecutive patients.
Lancet.
1998;352:1007-1011.
37.
Ellingson RJ, Wilken K, Bennett DR. Efficacy of sleep deprivation as an activation procedure in epilepsy patients.
J Clin Neurophysiol.
1984;1:83-101.
38.
Olson DM. Success of ambulatory EEG in children.
J Clin Neurophysiol.
2001;18:158-161.
39.
Devinsky O, Sato S, Kufta CV, et al. Electroencephalographic studies of simple partial seizures with subdural electrode recordings.
Neurology.
1989;39:527-533.
40.
Rosenow F, Wyllie E, Kotagal P, et al. Staring spells in children: descriptive features distinguishing epileptic and nonepileptic events.
J Pediatr.
1998;133: 660-663.
41.
Pachatz C, Fusco L, Vigevano F. Benign myoclonus of early infancy.
Epileptic Disord.
1999;1:57-61.
42.
Wulff CH, Ostergaard JR, Storm K. Epileptic fits or infantile masturbation?
Seizure.
1992;1:199-201.
43.
Panayiotopoulos CP. Elementary visual hallucinations, blindness, and headache in idiopathic occipital epilepsy: differentiation from migraine.
J Neurol Neurosurg Psychiatry.
1999;66:536-540.
44.
Haut SR, Bigal ME, Lipton RB. Chronic disorders with episodic manifestations: focus on epilepsy and migraine.
Lancet Neurol.
2006;5:148-157.
45.
Hart YM, Andermann F. Migraine aura, seizures, and temporal lobe epilepsy.
Adv Neurol.
1999;81:145-152.
46.
Lombroso CT. Pavor nocturnus of proven epileptic origin.
Epilepsia.
2000;41:1221-1226.
47.
Brower MC, Price BH. Epilepsy and violence: when is the brain to blame?
Epilepsy Behav.
2000;1: 145-149.
48.
Fleisher DR, Gornowicz B, Adams K, et al. Cyclic vomiting syndrome in 41 adults: the illness, the patients, and problems of management.
BMC Med.
2005;21:20.
49.
Shuper A, Goldberg-Stern H. Ictus emeticus(ictal vomiting).
Pediatr Neurol.
2004;31:283-286.
50.
Panayiotopoulos CP. Benign childhood epileptic syndromes with occipital spikes: new classification proposed by the International League Against Epilepsy.
J Child Neurol.
2000;15:548-552.
51.
Marcelli V, Piazza F, Pisani F, Marciano E. Neuro-otological features of benign paroxysmal vertigo and benign paroxysmal positioning vertigo in children: a follow-up study.
Brain Dev.
2006;28:80-84.
52.
Salvinelli F, Firrisi L, Casale M, et al. Benign paroxysmal positional vertigo: diagnosis and treatment.
Clin Ter.
2004;155:395-400.





Seizures could be the cause of many sudden unexplained deaths in toddlers
January 9th 2024The study authors noted that without video evidence, seizures would not have been implicated in death investigations and that seizure-related deaths are underrecognized in patients with epilepsy and in those without.

FDA warns of serious potential reaction to levetiracetam and clobazam
November 30th 2023The reaction, called Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), can start as a rash but can progress quickly, potentially resulting in injury to internal organs, hospitalization, and death.

Dietary therapies safe and efficient for treating drug-resistant epilepsy
February 7th 2023While treatment discontinuation because of adverse events was more likely when taking dietary therapies for treating childhood drug-resistant epilepsy, reduction of seizures and seizure freedom were significantly more common.



