





Gastrointestinal manifestations of cystic fibrosis: A primer for pediatricians
Significant improvements in cystic fibrosis (CF) care have focused primarily on the pulmonary system, but addressing the gastrointestinal complications of CF presents a major opportunity for improvement in disease management.


Table 1
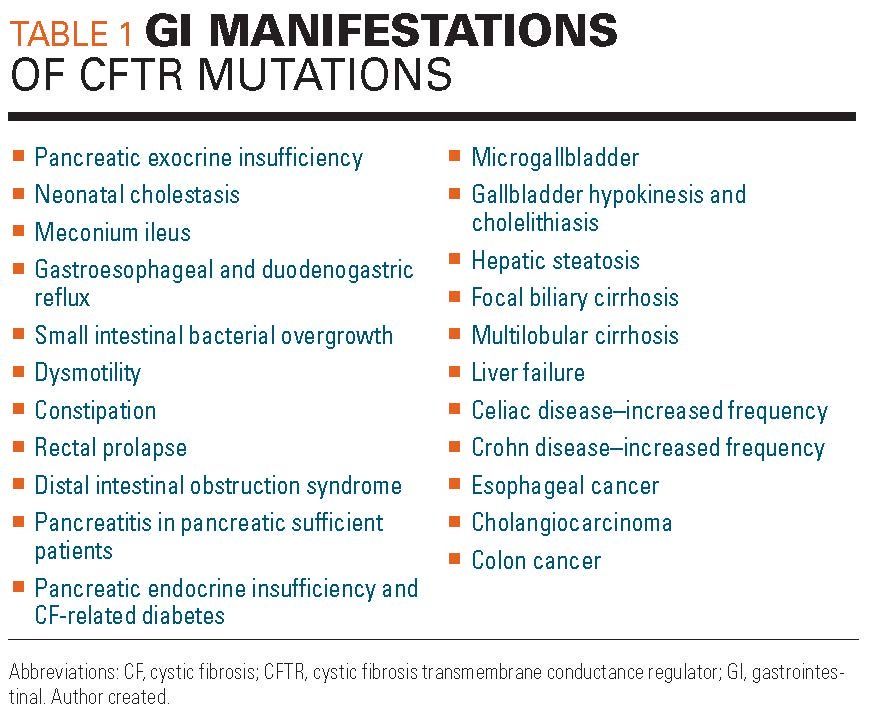


Figure 1a



Figure 1b



Table 2
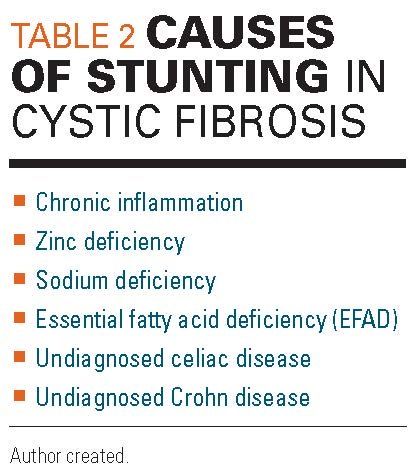


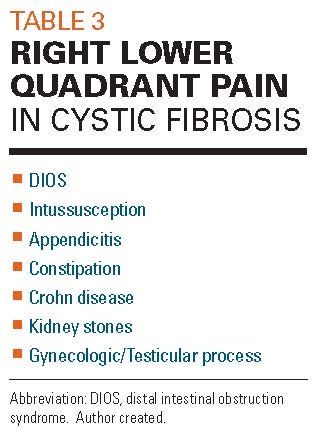
Table 3
Cystic fibrosis (CF) is the most common lethal autosomal recessive disease in the United States, occurring in 2000 to 4000 newborns.1 It is caused by one of the more than 2000 mutations of the CF transmembrane conductance regulator (CFTR). Although most of its morbidity and mortality stems from pulmonary decline, it was first recognized in 1938 as a cause of severe failure to thrive in infants due to characteristic pancreatic insufficiency. Decades later, we are starting to understand the full implication of the effects CFTR mutations on the entirety of the gastrointestinal (GI) system (Table 1).
The CFTR transports chloride and bicarbonate across the apical surface of epithelial cells in the respiratory and GI tracts. Mutations are classified as I to VI, with I to III being the most severe. Mutations result in abnormal structure, synthesis, and/or function of the CFTR protein.
Newborn screening detects trypsinogen, a protein released from the pancreas during the process of its destruction in utero. However, there are false negative results or cases where the specimen is unacceptable, or not received, and there is no appropriate follow-up. As 60% of infants are born with pancreatic insufficiency and another 30% will develop insufficiency in the next 3 years, and as GI, pancreatic, and hepatic manifestations are the most common initial manifestations of CF, before pulmonary manifestations become apparent, clinicians should have a low threshold for obtaining additional testing if CF is suspected.1
Nutrition
Achieving optimal growth in early life correlates with fewer pulmonary exacerbations and fewer hospitalizations.2 Infants with CF should be seen monthly to monitor proper growth and then every 3 months for routine care.3 Patients with suboptimal growth should be seen more frequently.
Children with CF require 110% to 200% of normal caloric intake to achieve normal growth.4 In general, the goal body mass index (BMI) is the 50th percentile for age, or the 50th percentile weight-for-length in children aged younger than 2 years. In instances where BMI offers a poor reflection of nutritional status, such as hepatomegaly or ascites, mid-arm circumference serves as an alternative measure. Attainment of nutritional goals involves adequate caloric intake, supplementation with fat-soluble vitamins (A, D, E, K), and pancreatic enzyme replacement therapy (PERT) under the guidance of a CF-trained nutritionist.
In addition to BMI, stunted height must be screened for, as height also correlates with lung function.5 There are multiple causes of stunting in CF (Table 2). A chronic inflammatory state makes insulin-like growth factor 1 (IGF1) less responsive to growth hormone. In addition, CF-related diabetes (CFRD), a unique form of diabetes specific to CF, can lead to growth failure.
Zinc deficiency from malabsorption and sodium deficiency related to CFTR dysfunction also can contribute to poor growth.3 Serum sodium may be normal despite depleted body sodium. A urine sodium to creatinine ratio can be measured. Cystic Fibrosis Foundation (CFF) guidelines emphasize sodium supplementation from infancy onward and with exercise. Zinc supplementation can be instituted empirically if a child is failing to thrive.
Due to fat malabsorption and dysregulation of fatty acid metabolism, patients with CF frequently have essential fatty acid deficiency (EFAD),6 which contributes to poor growth and can lead to immune system compromise, dermatitis, alopecia, and thrombocytopenia.
In young children, picky eating can lead to inadequate weight gain. Although often a behavioral issue, underlying pathology from eosinophilic or celiac disease can manifest as picky eating, so these should be considered. All patients and families should be screened for food insecurity.
Attainment of nutritional goals is important. If a child is failing to meet goals, early discussions around invasive interventions such as nasogastric, gastrostomy, gastrojejunal, or jejunal tubes should be undertaken, as families may need time to become comfortable with these ideas.
Gastrointestinal issues
PANCREATIC INSUFFICIENCY
Sixty percent of newborns with CF are born with complete pancreatic insufficiency (PI), and another 25% develop it by age 1 year.7 A baseline fecal elastase should be obtained in the neonatal period to assess for pancreatic sufficiency. Patients can develop PI at any time without early symptoms to indicate change. Annual monitoring with fecal elastase is recommended. A decrease in fecal elastase precedes steatorrhea. Steatorrhea develops only after lipase output falls below 10%. Fecal elastase can be falsely positive in watery stool and in severe nutritional depletion. In the latter case, testing should be repeated once nutritional repletion is addressed.
Pancreatic enzyme replacement therapy is critical to nutrient absorption and growth. It is important to optimize the timing of enzymes when the child is actively eating or immediately after, not prior to meals. Schools may need additional information about proper medication timing.
DYSMOTILITY: MECONIUM IIEUS (MI), INTUSSUSCEPTION, CONSTIPATION, AND DISTAL INTESTINAL OBSTRUCTION SYNDROME (DIOS)
Children with CF have an altered intraluminal intestinal environment. Gut microbiome changes in CF are already detected at 15 days of life.1 Breastfeeding can help promote diversity but does not eliminate all the issues related to CFTR dysfunction. This CFTR dysfunction leads to a dehydrated intestinal mucin layer and inspissated secretions. Decreased pancreatic bicarbonate secretion changes pH, and together with overexposure to acid reducers and antibiotics results in altered gut microbiota with diminished diversity, which can mimic a Crohn-like microbiome.8 The diminished diversity can lead to overgrowth of bacteria, impairing the enteric nervous system and contributing to slowed motility and stagnation.9,10
In the neonatal period this manifests as meconium ileus (MI), occurring in up to 25% of neonates with CF.11 Meconium ileus develops in utero and is characterized by thick meconium in the terminal ileum. Whereas MI may resolve on its own, it frequently presents with signs and symptoms of small bowel obstruction (SBO), such as vomiting, abdominal distention, and failure to pass meconium, and also can lead to microcolon. The patient’s X-rays will show dilated loops of bowel, sometimes with fluid levels and “soap bubbles” in the area of the meconium. Treatment is supportive with intravenous fluids and nasogastric decompression and includes surgical consultation. Hyperosmolar enema administration under fluoroscopy can dislodge meconium in 30% to 80%, although with risk of perforation it should be performed by an experienced radiologist.11 Up to 50% of cases of MI can be complicated by prenatal or segmental volvulus, ischemic necrosis, perforation, and intestinal atresia. All infants with MI should have an evaluation for CF. If the sweat test and trypsinogen are negative, infants should be referred for genetic testing.
Thickened intestinal secretions also predispose children with CF to intussusception, which has a prevalence of 1% and is most commonly ileocolonic.12 It is more common in older children with CF, contrary to healthy children. It may be the presenting complaint of undiagnosed CF.
Persistent constipation is also prevalent in this population. As a result, almost a quarter of CF patients have experienced rectal prolapse. Prolapse is rarely the initial presentation of CF, so consider other diagnoses (ie, Hirschsprung disease) first in the absence of other symptoms. However, with recurrent prolapse associated with diarrhea, evaluation for CF is warranted.1 Constipation must be differentiated from DIOS, which can present with acute right lower quadrant pain and signs and symptoms of SBO (Figure).
Distal intestinal obstruction syndrome is most common in older adolescents with a prevalence of 10% to 15.8%.13 The greatest risk factor is prior DIOS. In constipation, stool and gas accumulate gradually in the colon with or without colonic dilatation. Nonstimulant laxatives (ie, polyethylene glycol) are most commonly used for treatment of constipation and prevention of DIOS. Patients may require admission for nasogastric administration of the large volumes that are often needed (20-40 mL/kg/h) until effluent is clear. A gastrografin enema can be performed by a radiologist for treatment of DIOS.
If DIOS is refractory to standard treatments, alternate diagnoses should be considered, such as intermittent intussusception, ileal Crohn disease, or appendicitis. In CF, appendicitis mimics DIOS due to its atypical presentation with classic symptoms frequently absent. Interestingly, appendicitis occurs in 1% to 2% of children with CF compared with 7% of the non-CF population, likely because of the frequent use of antibiotics in CF. However, due to confusion with DIOS, perforation is more common.12
REFLUX
Sixty-seven percent of children with CF have reflux on impedance monitoring. Reflux is attributed to a variety of factors, including delayed gastric emptying; impaired gut motility; increased intra-abdominal pressure from coughing; effects of respiratory medications on the lower esophageal sphincter (LES) pressure; inherently decreased LES basal tone; hyperinflation of lungs with increased transdiaphragmatic pressure; abnormal esophageal peristalsis; postural drainage techniques in infants; and a high fat diet.14 Acid reducers increase the pH of refluxate but may not necessarily affect frequency of episodes of reflux unless the reflux is so severe that acid exposure has impaired the LES. Acid reducers should not be used indefinitely as they have been associated with small intestinal bacterial overgrowth and an increased risk of respiratory infections.
Altered motility also results in duodenogastroesophageal reflux, as demonstrated by increased bile in the stomachs of children with CF.14 Bile salts are an irritant and airway exposure correlates with worse lung disease. Erythromycin, which improves gastric emptying on scintinography in patients with CF, may offer benefit.
MICROBIOME CHANGES: SMALL INTESTINAL BACTERIAL OVERGROWTH (SIBO), CLOSTRIDIUM DIFFICILE
Small intestinal bacterial overgrowth (SIBO) can present with abdominal pain, bloating, and diarrhea as well as nutrient malabsorption.10 Providers should have a high index of suspicion for this diagnosis and treat empirically as the breath tests used in other populations are difficult to interpret in CF. Diagnosis should be under the guidance of a gastroenterologist.
Patients with CF have risk factors for acquisition of Clostridium difficile infections, including recurrent antibiotics use, hospitalization, dysbiosis, and acid reducer use. Asymptomatic carriage rates in CF are 22% to 55%.12 Diarrhea is uncommon. The presentation is often fulminant disease with rapid progression to toxic megacolon.
HEPATOBILIARY
Cholestasis is the earliest and most common manifestation of CF liver disease (CFLD), which is a diagnosis of exclusion. Cystic fibrosis liver disease is seen in 6% of infants with CF, but up to 25% of those with meconium ileus.1 Dysfunctional CFTR in cholangiocytes leads to inspissated bile and bile duct plugging. Additionally, up to one-third of neonates with CF have microgallbladder.15 Clinically, these findings can be confused with biliary atresia, which should be ruled out urgently. Infants with cholestasis benefit from a formula rich in medium-chain triglycerides, which do not require bile acids or micellular formation for absorption. Currently, there is no evidence supporting the routine use of ursodiol in CF.16 Cholestasis exacerbates fat-soluble vitamin malabsorption and leads to osteopenia, due to deficiency of vitamins D and K.15 Bone density scans are part of routine monitoring.
Gallbladder disease occurs in up to 50% of children with CF.15 In addition to microgallbladder, gallbladder hypokinesis is common as well. This predisposes patients to gallbladder stasis, which can lead to gallstones, with a prevalence up to 25%, including neonates. The evaluation and treatment are the same as for the general population and should be undertaken early in anticipation of progressive pulmonary operative risk over time. Biliary scintigraphy should be considered to evaluate emptying of the cystic duct, as bile duct strictures are not uncommon. Patients with biliary strictures are also at increased risk of cholangiocarcinoma.
Hepatic steatosis has a prevalence of 23% to 70% at any age.3 It is likely multifactorial, resulting from malnutrition; CFTR dysfunction; deficiencies of choline, carnitine, essential fatty acids; or poorly controlled CFRD.1 Other non–CF-related conditions also can result in steatosis. These patients should be referred to Gastroenterology.
Transient elevations of liver enzymes and gamma-glutamyl transferase (GGT) are exceedingly common and do not predict chronic liver disease.1,17 Elevations should be followed every 1 to 2 weeks until resolved or stable. Abnormalities persisting beyond 6 months should be evaluated with complete abdominal ultrasound with liver vascular duplex and referral to Gastroenterology. Hepatosplenomegaly should prompt earlier referral. Standard evaluation for chronic elevation of transaminases includes consideration of infectious hepatitis, drug-induced liver disease (from modulators, antibiotics, etc.), autoimmune hepatitis, Wilson disease, alpha-1-antitrypsin disease, and celiac disease.18
Cystic fibrosis liver disease is the 3rd-leading cause of death in CF following lung disease and transplant complications, and constitutes 2.5% of mortality in CF.16 Incidence increases every year from birth reaching 32% by age 25 years and then levels out. There is a higher prevalence among males, those homozygous for F508del, and those with a history of meconium ileus. Synthetic function is usually preserved. Cystic fibrosis liver disease is thought to be a consequence of bile ductule inspissation that starts out as areas of focal biliary cirrhosis with progression to multilobular cirrhosis and a nodular liver on exam. Five percent to 10% of patients have multilobular cirrhosis before adolescence.18 The most significant consequence of CFLD is progression to portal hypertension, which can lead to varices and hypersplenism. Regular use of nonsteroidal anti-inflammatory drugs (NSAIDs) should be avoided in this context due to resultant thrombocytopenia. Varices are treated with banding, and transjugular intrahepatic portosystemic shunt is considered with recurrent bleeding as bridge to liver transplantation.
Development of ascites is an ominous sign usually accompanied by a decline in nutrition and lung function.18 Signs of impending liver failure include declining platelets, hypoalbuminemia, elevated international normalized ratio (INR), and hypoglycemia. Hepatopulmonary syndrome is a rare but serious complication with a 5-year survival rate of 23%.
ABDOMINAL PAIN
In healthy children, the frequency of occasional abdominal pain is about 11%. In contrast, 50% to 60% of children with CF report chronic abdominal pain.12 This is a major issue for quality of life, leading to sleep disruption, restriction of activities, and contributing to anxiety and depression. Functional abdominal pain is common due to visceral hyperalgesia and amplification of pain attributed to the stress of being chronically ill. Additional considerations include gastritis (due to frequent use of steroids or NSAIDs), pancreatitis (among patients who have pancreatic sufficiency),19 and postoperative complications, such as adhesions or strictures following abdominal surgery. Right upper quadrant or epigastric pain should alert a provider to the possibility of cholelithiasis.
There is a 3-fold increased prevalence of celiac disease in CF, but it often goes unrecognized.20 However, CF alone can result in a falsely elevated anti-tissue transglutaminase (tTG) immunoglobulin A (IgA), as it is an acute phase reactant.12 Thus, endoscopic evaluation is necessary to confirm celiac disease.
Right lower quadrant pain can be due to appendicitis, DIOS, intussusception, or Crohn disease, which is 17 times more prevalent in CF than the general population21 (Table 3). As in children without CF, intermittent abdominal pain can be due to undiagnosed malrotation with intermittent volvulus. In particular, infants with CF are at higher risk of volvulus in absence of malrotation due to inspissation of meconium. Fat malabsorption increases the risk of oxalate kidney stones.
Gynecologic or testicular issues also should be remembered in the appropriate clinical settings.
Conclusion
Significant improvements in CF have focused primarily on the pulmonary system with less attention given to the gastrointestinal complications.22,23 Effects of CFTR mutations on the gastrointestinal system are beginning to be better appreciated. The complex interplay between electrolytes, enzymes, microbiota, and the various other components of gut physiology requires further research.
Gastrointestinal symptoms contribute substantially to morbidity in CF and represent a major opportunity for improvement in the care of these patients. A multidisciplinary team of pediatricians, pulmonologists, gastroenterologists, respiratory therapists, nutritionists, pharmacists, and physical therapists who appreciate the complexity of this disease and recognize the importance of the holistic approach in patients’ care can make a significant difference in these children’s life expectancy and quality of life.
References:
1. Galante G, Freeman AJ. Gastrointestinal, pancreatic, and hepatic manifestations of cystic fibrosis in the newborn. NeoReviews. 2019;20(1):e12-e24.
2. Hauschild DB, Rosa AF, Ventura JC, et al. Association of nutritional status with lung function and morbidity in children and adolescents with cystic fibrosis: a 36-month cohort study [article in English, Portuguese]. Rev Paul Pediatr. 2018;36(1):8.
3. Sullivan JS, Mascarenhas MR. Nutrition: Prevention and management of nutritional failure in cystic fibrosis. J Cyst Fibros. 2017;16 suppl 2:S87-S93.
4. Stallings VA, Stark LJ, Robinson KA, et al; Clinical Practice Guidelines on Growth and Nutrition Subcommittee; Ad Hoc Working Group. Evidence-based practice recommendations for nutrition-related management of children and adults with cystic fibrosis and pancreatic insufficiency: results of a systematic review. J Am Diet Assoc. 2008;108(5):832-839.
5. Sheikh S, Zemel BS, Stallings VA, Rubenstein RC, Kelly A. Body composition and pulmonary function in cystic fibrosis. Front Pediatr. 2014;2:33.
6. Freedman SD, Blanco PG, Zaman MM, et al. Association of cystic fibrosis with abnormalities in fatty acid metabolism. N Engl J Med. 2004;350(6):560-569.
7. Singh VK, Schwarzenberg SJ. Pancreatic insufficiency in cystic fibrosis. J Cyst Fibros. 2017;16 suppl 2:S70-S78.
8. Enaud R, Hooks KB, Barre A, et al. Intestinal inflammation in children with cystic fibrosis is associated with Crohn’s-like microbiota disturbances. J Clin Med. 2019;8(5):E645.
9. Rogers GB, Narkewicz MR, Hoffman LR. The CF gastrointestinal microbiome: structure and clinical impact. Pediatr Pulmonol. 2016;51(S44):S35-S44.
10. Dorsey J, Gonska T. Bacterial overgrowth, dysbiosis, inflammation, and dysmotility in the cystic fibrosis intestine. J Cyst Fibros. 2017;16 suppl 2:S14-S23.
11. Sathe M, Houwen R. Meconium ileus in cystic fibrosis. J Cyst Fibros. 2017;16 suppl 2:S32-S39.
12. Lusman SS, Grand R. Approach to chronic abdominal pain in cystic fibrosis. J Cyst Fibros. 2017;16 suppl 2:S24-S31.
13. Abraham JM, Taylor CJ. Cystic fibrosis & disorders of the large intestine: DIOS, constipation, and colorectal cancer. J Cyst Fibros. 2017;16 suppl 2:S40-S49.
14. Maqbool A, Pauwels A. Cystic fibrosis and gastroesophageal reflux disease. J Cyst Fibros. 2017;16 suppl 2:S2-S13.
15. Assis DN, Debray D. Gallbladder and bile duct disease in cystic fibrosis. J Cyst Fibros. 2017;16 suppl 2:S62-S69.
16. Boëlle P, Debray D, Guillot L, et al: French CF Modifier Gene Study Investigators. Cystic fibrosis liver disease: outcomes and risk factors in a large cohort of French patients. Hepatology. 2019;69(4):1648-1656.
17. Woodruff SA, Sontag MK, Accurso FJ, Sokol RJ, Narkewicz MR. Prevalence of elevated liver enzymes in children with cystic fibrosis diagnosed by newborn screen. J Cyst Fibros. 2017;16(1):139-145.
18. Leung DH, Narkewicz MR. Cystic fibrosis-related cirrhosis. J Cyst Fibros. 2017;16 suppl 2:S50-S61.
19. Freeman AJ, Ooi CY. Pancreatitis and pancreatic cystosis in cystic fibrosis. J Cyst Fibros. 2017;16 suppl 2:S79-S86.
20. Fluge G, Olesen HV, Gilljam M, et al. Co-morbidity of cystic fibrosis and celiac disease in Scandinavian cystic fibrosis patients. J Cyst Fibros. 2009;8(3):198-202.
21. Lloyd-Still JD. Crohn’s disease and cystic fibrosis. Dig Dis Sci. 1994;39(4):880-885.
22. Middleton PG, Mall MA, DÅevÃnek P, et al; VX17-445-102 Study Group. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single Phe508del allele. N Engl J Med. 2019;381(19):1809-1819.
23. Taylor-Cousar JL, Munck A, McKone EF, et al. Tezacaftor-ivacaftor in patients with cystic fibrosis homozygous for Phe508del. N Engl J Med. 2017;377(21):2013-2023.























The Role of the Healthcare Provider Community in Increasing Public Awareness of RSV in All Infants
April 2nd 2022Scott Kober sits down with Dr. Joseph Domachowske, Professor of Pediatrics, Professor of Microbiology and Immunology, and Director of the Global Maternal-Child and Pediatric Health Program at the SUNY Upstate Medical University.



