





Viral croup: Current diagnosis and treatment
Croup sometimes resembles more serious disease, and management options range from home treatment with mist to PICU admission. The authors explain how to recognize viral croup, review the latest studies on when to use nebulized or systemic steroids, and suggest common-sense criteria for hospitalization.
Viral croup: Current diagnosis and treatment
By Athanasios G. Kaditis, MD, and Ellen R. Wald, MD
Croup sometimes resembles more serious disease, and managementoptions range from home treatment with mist to PICU admission. The authorsexplain how to recognize viral croup, review the latest studies on whento use nebulized or systemic steroids, and suggest common-sense criteriafor hospitalization.
There has been substantial debate regarding optimal medical managementof viral croup, a common childhood disease. The clinical manifestationsof croup may be confused with the presentation of more serious diseasessuch as epiglottitis and bacterial tracheitis. This article summarizes thecurrent knowledge regarding diagnosis and management of croup.
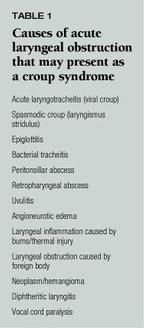
The term croup describes a syndrome characterized by a bark-like cough,hoarseness, inspiratory stridor, and respiratory distress of varying severity.In 1950 a classification was proposed for the several different pathologicconditions causing acute laryngeal obstruction. These disorders may presentwith all or with most of the manifestations of the croup syndrome (Table1).


The most common and most typical form of the croup syndrome is acutelaryngotracheitis. This infection, which is caused by a virus, is usuallypreceded by coryza and low-grade fever for 12 to 72 hours. Incidence ofthe disease is highest in the second year of life, and it decreases substantiallyafter the sixth year. Parainfluenza viruses (types 1, 2 and 3) are the mostfrequent etiologic agents, but respiratory syncytial virus, influenza virus,and adenovirus may also be responsible for laryngotracheitis. These virusescause inflammation affecting the subglottic tissues and sometimes the trachealmucosa.
In contrast to acute laryngotracheitis, epiglottitis is characterizedby inflammation of the supraglottic tissues and is caused mainly by Haemophilusinfluenzae type b. A previously healthy child, usually between 2 and 4 yearsof age, suddenly develops a sore throat and fever. Within hours after theonset of symptoms, the patient looks toxic, swallowing is painful, and breathingis difficult. Drooling is frequently present, while the neck is hyperextendedin an attempt to keep the airway open.
Viral croup may be complicated by bacterial tracheitis caused by Staphylococcusaureus, H influenzae, Streptococcus pneumoniae or Moraxella catarrhalis.Although the supraglottic tissues in bacterial tracheitis usually appearnormal, the tracheal mucosa may be ulcerated and partly necrotic and isfrequently covered by a thick, purulent exudate. A child with bacterialtracheitis may present in two ways. One presentation resembles viral croup.However, after several days, usually when the child has begun to improve,high fever, toxicity, and increasing respiratory distress (which do notrespond to the usual treatment for viral laryngotracheitis) develop. Endotrachealintubation is usually required. In the other presentation the viral prodromeis absent, and the initial clinical features are similar to those of acuteepiglottitis (high fever and increased respiratory effort), although thepatient does not drool.
Spasmodic croup (laryngismus stridulus) presents with a clinical picturesimilar to that of viral croup except that the nasal symptoms are less prominent.The symptoms of spasmodic croup start suddenly in the middle of the night,often without any preceding signs or only modest signs of an upper respiratoryinfection. Exposure to the cold night air may alleviate the symptoms, butsome children require airway support. Recurrences may be observed for severalnights in a row. The etiology of spasmodic croup is unclear. Pale, edematousmucosa of the subglottic area with a boggy appearance may be the cause oflaryngeal obstruction in some cases. Spasm of the glottis with closure ofthe ventricular bands and crowded aryepiglottic folds may be responsiblefor spasmodic croup in other cases.
Diagnostic aids in viral croup
Radiographic studies. Radiographs of the neck have been used toconfirm the diagnosis of laryngotracheitis and exclude other causes of thecroup syndrome. In a typical case the frontal view will show narrowing ofthe laryngeal air column for about 5 to 10 mm below the level of the vocalcords caused by mucosal edema (steeple sign). The lateral film may revealoverdistention (ballooning) of the hypopharynx during inspiration.
The benefit of the performance of the neck radiographs in differentiatingbetween viral croup, epiglottitis and bacterial tracheitis has been controversial.The steeple sign on the frontal neck radiograph may be absent in some childrenwith croup, may be present in children without croup (as a normal variant)and has also been reported to occur in patients with epiglottitis. Neckradiographs in eight of 30 patients with a clinical diagnosis of laryngotracheitisand in six of 21 patients with head trauma and no respiratory disease wereinterpreted as "positive for" or "cannot rule out" epiglottitis.1,2Furthermore, in patients who are suspected on clinical grounds to have epiglottitis,the performance of the lateral neck radiograph may simply delay appropriatemanagement of the airway. On the other hand, investigators from the Children'sHospital of Philadelphia, using lateral neck roentgenograms, claim a sensitivityof 93% and a specificity of 92% for the diagnosis of viral laryngotracheitis.3
Despite this claim, we believe that the diagnosis of viral croup restson clinical grounds and does not require a radiograph of the neck.
Pulse oximetry. A study from the United Kingdom showed a poorcorrelation of clinical status and respiratory rate with hypoxia.4In that study, frequent decreases in oxygen saturation were caused by movementartifacts. Observation and frequent physical examinations remain the mostaccurate way to monitor a child with acute laryngotracheitis. Pulse oximetrymay be more useful if the patient also has bronchiolitis or pneumonitis.
Direct inspection of oral cavity and oropharynx in the emergency department.There is general agreement that the patient in whom complete obstructionof the airway is imminent needs laryngoscopy and airway support in a well-controlledenvironment. Different institutions use different protocols, but in generalthe child is transferred in a calm reassuring manner to the intensive careunit or to the operating room. A volatile anesthetic is administered througha face mask and then laryngoscopy and endotracheal intubation are performed.Bronchoscopy is conducted if indicated.5 In children with a lessdramatic presentation of obstruction of the upper airway, examination ofthe oral cavity and oropharynx in the emergency department will excludecertain entities that may mimic the presentation of epiglottitis, such asa peritonsillar or a retropharyngeal abscess or uvulitis.
The safety of direct inspection of the oral cavity and oropharynx inthe emergency department has been controversial; there have been concernsthat even in patients with mild respiratory distress, examination of theairway may precipitate complete obstruction. These concerns, arising inan era when epiglottitis was a more common infection, are not supportedby clinical experiences that have been published. There have been only tworeports of children with acute epiglottitis who experienced complete airwayobstruction after direct inspection of the epiglottis. The circumstancesbefore and during the examination are not described in detail; accordinglyit is impossible to know whether complete airway obstruction was a complicationof the direct inspection of the epiglottis or the result of the naturalcourse of the infection. Diaz and Lockhart described 104 children with epiglottitis,and Mauro et al described 149 children with viral croup and six with epiglottitis,all of whom underwent direct inspection of the oropharynx without adverseeffects.6,7 The diagnosis would have been missed in two of thesix children with epiglottitis in the series by Mauro et al if the clinicalimpression had been relied on.
Diagnostic endoscopy. The indications for endoscopy in patientswith laryngotracheitis are not well-defined. In two large series of patientswith laryngotracheitis, endoscopy was performed infrequently. In the studyfrom the Hospital for Sick Children in Toronto series, the authors suggesta very conservative approach, because instrumentation of the already edematoussubglottic area may precipitate the need for intubation.8 Thereforethey reserve endoscopy for children who have historical evidence suggestiveof a diagnosis other than viral croup: noisy breathing or an abnormal crybetween episodes of croup; progressively more severe or frequent episodesof croup; intubation in the neonatal period; and choking or gagging beforethe onset of symptoms.8,9
Investigators from Montreal Children's Hospital recommend endoscopy forchildren with croup severe enough to require intubation or for those withan atypical history or clinical manifestations (age older than 3 years,recurrent croup, history of laryngeal nerve injury, minimal response totreatment).10 Endoscopy of the airway should be also consideredin patients who present with symptoms that are consistent with bacterialtracheitis. Bronchoscopy can be extremely helpful in collecting secretionsfrom the lower airway for bacterial cultures,so that antimicrobial treatmentcan be directed against specific pathogens.
Is viral laryngotracheitis a life-threatening disease?
Viral croup in general is considered a benign self-limited disease. However,hospitalization rates of 20 to 24.3% (of patients seen at the emergencydepartment) and rates of intubation between 1.6% and 3.2% (of hospitalizedpatients) were reported before the more extensive use of systemic steroids.79,11
Influenza A2 virus may cause severe croup with a substantial number ofpatients requiring airway management. In addition, the reappearance of bacterialtracheitis, as a complication of viral croup, is another reason why childrenmay require intubation.
There is only a single study that reports on the progression of symptomsin children who are admitted to the hospital with the diagnosis of virallaryngotracheitis.12 Patients were categorized into three gradesof clinical severity: Grade 1 patients had stridor at rest without retractions;Grade 2 patients had stridor and retractions (sternal and chest wall); andGrade 3 patients were in marked respiratory distress indicated by irritability,pallor or cyanosis, tachycardia, and exhaustion. All patients were admittedto the hospital, but Grade 1 and Grade 2 patients did not receive any typeof treatment initially. Of patients with croup of Grade 1 in severity, 11%deteriorated and required treatment with cool mist and/or racemic epinephrine.Of patients with croup of Grade 2 in severity, 49% developed worse symptomsand were treated with cool mist and/or racemic epinephrine. Of the subjectswho presented to the emergency department with Grade 3 symptoms, 53% wereintubated despite the use of cool mist and racemic epinephrine.
Treatment
Cool mist. The use of mist was introduced in the 19th centurywhen physicians observed that steam from teapots and hot tubs at home alleviatedthe symptoms of croup. Croup kettles were the first devices used for misttreatments. The risk of burns and the observation that the cold night airis also beneficial led to the modern devices that blow cool mist into acroup tent.
There are only two studies that have tested the efficacy of moist airin patients with croup and neither of them documented a significant benefit.The major weakness of both studies was the small sample size. In 1994 astudy from Sweden comparing nebulized racemic epinephrine with nebulizedsaline solution showed a statistically significant improvement in the croupsymptoms after administration of the saline solution.13 Unfortunatelythere was no group of patients for comparison who did not receive any therapeuticintervention. Improvement can also be explained by spontaneous recoverywith time.
Three mechanisms have been proposed to explain the potential beneficialeffect of cool mist: (1) cool mist moistens secretions (thereby facilitatingclearance); (2) the mist may activate mechanoreceptors in the larynx thatproduce a reflex slowing of respiratory flow rate (evidence from kittens);and (3) a feeling of comfort and reassurance provided to the child by theparent who holds him or her near the mist may prevent hyperventilation resultingfrom anxiety. Although cool mist is usually viewed as a simple and safemeasure to relieve the symptoms of croup, there are potential risks associatedwith its administration. Humidity can intensify bronchospasm in childrenwho have croup and wheezing at the same time. In addition, the system fordelivery of the mist may also influence its usefulness. The plastic tent,if used, separates the child from both the parents and the nursing staff.This may mean more anxiety for the young child and therefore increased respiratorydistress. The nursing staff on the other hand may miss signs of deteriorationin a young patient who is covered with a water fog. The best way to providemist is by a tube held in front of the patient by the parent. Children withwheezing may have a trial of cool mist. If the wheezing increases, the treatmentshould be discontinued.
Nebulized epinephrine. Between 1937 and 1964 hospitalization ofpatients with viral laryngotracheitis was associated with tracheotomy ratesbetween 2.9 and 13% and mortality rates between 0.09 and 2.7%. In 1971 Adairet al presented their 10-year experience with viral laryngotracheitis atPrimary Children's Hospital in Salt Lake, UT.14 None in a seriesof 351 patients hospitalized for viral croup either underwent tracheotomyor died. These excellent results were attributed to the administration ofnebulized racemic epinephrine with intermittent positive pressure breathingto all patients who were candidates for tracheotomy before the procedurewas performed. The authors also noted that up to one third of children treatedwith racemic epinephrine in the emergency department had been dischargedto home.
Racemic epinephrine is a 1:1 mixture of the d and l isomers of epinephrine.The l isomer causes constriction of the precapillary arterioles via stimulationof the alpha-receptors and thereby decreases capillary hydro static pressure.The final result is fluid resorption from the interstitial space (insteadof capillary leakage) and resolution or improvement of the laryngeal mucosaledema.
Subsequent studies confirmed the findings by Adair et al and demonstratedthat racemic epinephrine was equally effective whether it was deliveredby intermittent positive pressure breathing or by simple nebulization. Thedose of racemic epinephrine used in various studies was between 0.25 and0.75 mL of a 2.25% solution.15,16 Initially racemic epinephrinewas used in preference to the l isomer of epinephrine because it was thoughtto be associated with fewer side effects (tachycardia, hypertension) thanl-epinephrine. Waisman et al reported that equal doses of the active l form,given either alone or as the racemic mixture, had the same beneficial andadverse effects.17 This finding is of great practical importancebecause racemic epinephrine is not readily available outside of the UnitedStates. The only concern that has been raised about the l isomer is itspotential to cause irritation of the respiratory epithelium by the metabisulfitethat is contained in the medication solution.18 The dose usedin the study by Waisman et al was 5 mL of l-epinephrine at 1:1000.17To dilute the irritating substances contained in the epinephrine preparation,normal saline for nebulization can be added to the preparation.
Very early after the introduction of nebulized epinephrine by Adair etal, it was recognized that the action of the medication was limited to twohours or less. Adrenaline is rapidly metabolized by two enzymes (catechol0-methyltransferase and monoamine oxidase). Several authors emphasized thefact that the medication did not change the natural history of croup. Accordinglyit was recommended that children requiring administration of racemic epinephrineshould be hospitalized in case the symptoms reappeared after the activityof the epinephrine had diminished. The recurrence of the initial clinicalpicture has been described as a "rebound phenomenon."
Administration of nebulized epinephrine to children with croup in theemergency department became a major indication for admission to the hospitalin the 1980s.19 Recently these recommendations have been reassessed.It seems to be safe to dismiss a child who received nebulized adrenalinefrom the Emergency Department if, after three to four hours of observation,the child has (1) no stridor at rest, (2) normal air entry, (3) normal coloror (4) normal level of consciousness and has received one dose of 0.6 mg/kgdexamethasone, orally or intramuscularly. 15,16,20
In most studies racemic epinephrine has been administered to childrenwith moderate to severe viral croup. The possible explanation for the dramaticdecrease of tracheotomies reported since the introduction of racemic epinephrinemay relate to its provision of temporary relief which provides time eitherfor the steroids to work or for the disease to run its natural course towardspontaneous resolution.21 Severe laryngeal obstruction is anindication for the use of epinephrine before attempting intubation (providedthat the airway is not completely obstructed and there is still time fora trial of medication). Likewise its use is justified in patients who havesevere retractions because it provides temporary relief to an uncomfortablepatient, while waiting for an expected recovery or for the arrival of anindividual who is skilled at intubation. Administration of nebulized epinephrineto children with viral laryngotracheitis who do not have signs of respiratorydistress is unnecessary.
Parenteral and oral corticosteroids. After decades of debate aboutthe potential beneficial effect of systemic corticosteroids in patientswith viral croup, there is now ample evidence to support their use in patientswith severe, moderate, or even mild croup. Corticosteroids exert their beneficialeffect by decreasing edema of the laryngeal mucosa via their anti-inflammatoryaction. Clinical improvement is usually not apparent until six hours aftertreatment, although in one study a decrease in severity of symptoms wasnoted within two hours of receipt of treatment with dexamethasone.22,23
In children who were intubated for severe viral laryngotracheitis, prednisolone1 mg/kg administered via a nasogastric tube every 12 hours and until 24hours after extubation reduced the duration of intubation and the need forreintubation.24
Several studies have also shown the efficacy of corticosteroids in patientswith viral laryngotracheitis of mild to moderate severity, who were observedin the emergency department or admitted to the hospital.11,2528Dexamethasone at 0.3 to 0.6 mg/kg, given either orally or intramuscularlyas a single dose, decreased: (1) the severity of symptoms in the treatedgroup compared with those who received placebo11,2628 (2)the need for subsequent treatments with nebulized epinephrine27(3) the number of patients admitted to the hospital after observation inthe emergency department11 (4) the number of patients transferredto the intensive care unit11 (5) the number of children requiringintubation;11,26and (6) the duration of hospitalization or observationin the emergency department.11,25
A recent clinical trial assessed the efficacy of 0.15 mg/kg dexamethasonecompared with placebo given orally in children with mild viral croup (nostridor or chest wall retractions at rest) who were discharged to home fromthe emergency department.29 This small single dose was effectivein reducing the number of children who returned to the emergency departmentfor further care.
Different doses and routes of administration for corticosteroids havebeen proposed. Dexamethasone 0.15 mg/kg is as effective as 0.3 or 0.6 mg/kgin relieving symptoms of viral laryngotracheitis of mild to moderate severity.25The oral and the intramuscular routes have been used in clinical trialsand have resulted in significant improvement compared with placebo. However,there is no study comparing directly the efficacy of oral vs. parenteralcorticosteroids.
Only a single adverse effect has been described after the use of systemiccorticosteroids for viral laryngotracheitis. A 14-month-old patient withviral croup developed laryngotracheitis caused by Candida albicans afteran eight-day course of dexamethasone (1 mg/kg/day) and antibiotics.30Clinical improvement in mild to moderate croup can usually be achieved witha much smaller single dose of corticosteroid, which is unlikely to causeserious side effects. Corticosteroids should not be administered to childrenwith varicella or tuberculosis (unless the patient is receiving appropriateantituberculous therapy) because they are associated with a severe clinicalcourse of these diseases.31 Finally, the clinician must rememberthat the potent effects of corticosteroids may mask the presentation ofan underlying process like an airway hemangioma.32
Nebulized corticosteroids. In 1993 Husby et al proposed that,at least theoretically, inhaled steroids should be advantageous in croup,because the active substance can reach the inflamed laryngeal tissue rapidlyand with minimal constitutional effects.33 Budesonide is a glucocorticoidwith high potency (when administered topically) and negligible systemiceffects. In their double blind, placebo-controlled study, the authors used2 mg of nebulized budesonide in children who were admitted to the hospitalwith moderate to severe croup. During a two-hour period they noted a significantimprovement in stridor and cough in the group that was treated. A secondtrial with patients of similar clinical severity used 2 mg of nebulizedbudesonide initially and then 1 mg every 12 hours.34 Childrenwho received budesonide had a significant improvement in symptoms and shorterhospital stay compared with children who received placebo.
Klassen et al studied nebulized budesonide (2 mg) for children with mildto moderate croup in the emergency department.35 At the end ofa four-hour assessment period patients in the treated group improved moreand were discharged to home earlier than the group who did not receive treatment.An improvement in clinical symptoms four hours after the administrationof 10 to 20 mg of nebulized dexamethasone has also been reported, but withouta concomitant decrease in the rates of hospitalization.36
Nebulized budesonide is as effective as oral dexamethasone in the managementof children hospitalized for viral laryngotracheitis.23 The additionof nebulized budesonide (2 mg) to a regimen of oral dexamethasone (0.6 mg/kg)for outpatients with croup enhanced recovery compared with oral dexamethasonealone.37
The beneficial effect of nebulized budesonide occurred within two tofour hours after treatment.34 This rapid onset of action withinhaled steroids is in contrast to the rather slow onset of action of systemicsteroids.22 Similar results have been described in asthmaticswho received large dosages of inhaled steroids.38,39 This effectmay be due to local vasoconstriction in the edematous laryngeal mucosa.40However, the same rapid action was recently reported for oral dexamethasoneadministered to inpatients with viral croup.23 If the route ofadministration (oral vs. inhaled) results in similar clinical results andthe onset of action is the same for both nebulized budesonide and oral dexamethasone,it is apparent that dexamethasone should be the corticosteroid of choicefor viral laryngotracheitis, given its much lower cost.
Endotracheal intubation. Endotracheal intubation has replacedtracheotomy in the management of severe airway obstruction secondary toviral laryngotracheitis. The decision to intubate is based on clinical criteriathat include increasing stridor, respiratory rate, heart rate, retractions,the appearance of cyanosis, exhaustion, confusion, or a failure to respondto nebulized epinephrine. Anesthesia is induced with oxygen and halothanethrough a face mask.5 Generally a tube with a diameter of 0.5to 1 mm less than the predicted size of the trachea for the child's ageis recommended.41 Intubated children should be admitted to anintensive care unit for observation and frequent suctioning to prevent obstructionof the endotracheal tube. The child is usually extubated when there is asignificant air leak around the tube at a positive airway pressure of about25 cm H2O.
Alternatively, at some medical centers children with viral croup andsevere airway obstruction have been treated with a mixture of helium andoxygen (70% to 80% concentration of helium) instead of room air or pureoxygen. Helium is an inert, nontoxic gas. Because of its low density andviscosity, it can move through the airways, causing less turbulent flowand with less resistance. Therefore the mechanical work of the respiratorymuscles, which must overcome the high resistance of the stenotic subglotticspace, decreases significantly. Patients with severe croup who breathe amixture of helium and oxygen become more comfortable and may avoid intubation.
Conclusions and recommendations
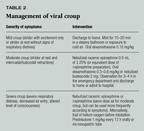
There are different levels of care for patients with viral croup, dependingon their clinical presentation. Children with mild symptoms (stridor withexcitement or stridor at rest without intercostal or subcostal retractions)can be safely managed at home with either mist provided for 15 to 20 minutesin a steamy bathroom or exposure to cold air outside the house. If the symptomsare of moderate severity (stridor at rest and intercostal or subcostal retractions),the child can either be discharged to home after observation for severalhours in the emergency department (to ensure an improving clinical status)or admitted to the hospital. Nebulized epinephrine may be used to relieveairway edema and respiratory distress.
Severely affected patients (severe respiratory distress, decreased airentry into the lungs, altered level of consciousness) are preferably admittedto a pediatric intensive care unit to receive treatments with nebulizedepinephrine and possible intubation. Offering a mixture of helium and oxygeninstead of room air may alleviate respiratory distress and prevent endotrachealintubation. Recent studies have emphasized the beneficial effect of usingsystemic and/or nebulized steroids in viral croup irrespective of the severityof symptoms (Table 2). Common-sense criteria for admission to the hospitalapply to children with viral croup and include signs of toxicity, poor oralintake leading to dehydration, age younger than 6 months, unreliable caregivers,or a family that lives a long distance from the hospital.


THE AUTHORS:
DR. KADITIS was a Fellow, Division of Allergy, Immunology,and Infectious Diseases, Department of Pediatrics, Children's Hospital ofPittsburgh, PA, when this article was written.
DR. WALD is Professor of Pediatrics, University of PittsburghSchool of Medicine, and Chief of the Division of Allergy, Immunology, andInfectious Diseases, the Children's Hospital of Pittsburgh.
This article is reprinted from Pediatric Infectious DiseaseJournal 1998;17:827834.
Viral croup: Current diagnosis and treatment. Contemporary Pediatrics 1999;0:139.



















