





Asymptomatic Girl Who Passes Threadlike Object in Stool
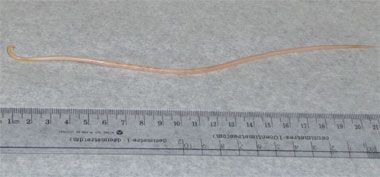
A healthy 4-year-old girl passed a threadlike object in her stool at a day-care center. She had no diarrhea, vomiting, or abdominal pain. Stool had no blood or melena. Child’s appetite normal.


HISTORY
A healthy 4-year-old girl passed a threadlike object in her stool at a day-care center. She had no diarrhea, vomiting, or abdominal pain. Stool had no blood or melena. Child’s appetite normal.
Patient born in Canada of a middle-class family. No history of traveling.
PHYSICAL EXAMINATION
Active, alert, well-nourished patient. Height, 101 cm (50th percentile); weight, 15.2 kg (25th percentile). Physical findings normal. In particular, no excoriation noted in the perianal area. No signs of anemia.
WHAT’S YOUR DIAGNOSIS? (Answer on next page)
ANSWER: ASCARIASIS
Ascariasis is caused by Ascaris lumbricoides, which enters the host by ingestion of eggs found in fecally contaminated material.1-4 In most patients, the roundworm infection is asymptomatic. In symptomatic patients, clinical manifestations can vary widely.


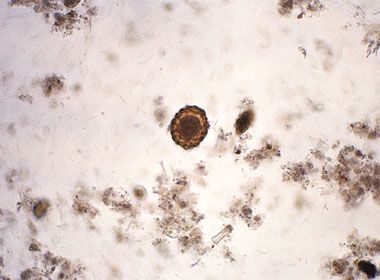
Figure – This photomicrograph shows a fertile Ascaris lumbricoides egg (magnification x128).
EPIDEMIOLOGY
Ascariasis is the most common helminthic infection in humans.5 About 1 billion people have ascariasis worldwide, of which 4 million cases are in the United States.6 Ascariasis has high endemicity in tropical and subtropical areas.3 Predisposing factors include poor socioeconomic conditions, use of human feces as fertilizer, and geophagia. Prevalence is greatest in children aged 2 to 10 years and decreases after 15 years of age.7 The incidence and intensity of infection is the same in males and females.2
ETIOLOGY
The embryonated eggs of A lumbricoides become infective after 10 to 15 days at 30°C or about 50 days at 17°C in moist soil, where they can remain viable for up to 2 years.6 When a mature egg (Figure) comes into contact with bile acids, the larva exits the egg case and burrows through the intestinal mucosa. The larva migrates to the liver via the hepatic portal circulation; then passes through the lungs, trachea, and epiglottis; and finally reenters the GI tract where it matures.4 New eggs (up to 20,000 a day per adult female worm) are released into the feces to complete the cycle. This process takes 9 to 11 weeks from egg ingestion.4
A lumbricoides-the largest intestinal nematode parasite in humans-can grow to 35 cm in length and 0.5 cm in thickness.8 An adult worm has a life span of 10 to 24 months.1
CLINICAL MANIFESTATIONS
Symptomatic patients tend to have higher worm loads and may present with vague abdominal or respiratory tract symptoms. The worms may be passed in feces or escape through the anus.4
COMPLICATIONS
In the larval stage, the main clinical complication is pulmonary ascariasis. An acute transient pneumonitis (Lffler syndrome) associated with fever, coughing, wheezing, dyspnea, hemoptysis, pulmonary infiltrates, and marked eosinophilia may occur.1
When the worms reach the adult phase, a greater variety of clinical complications may result. Intestinal ascariasis can cause nausea, vomiting, epigastric pain, abdominal discomfort, and diarrhea.9 Intestinal obstruction may result from worm bolus, small-bowel volvulus, or intussusception.4 Intestinal obstruction is more frequent in children because of their smaller intestinal lumens.4 Other intestinal complications include bowel perforation, peritonitis, and appendicitis. A chronic granulomatous peritonitis can also occur if an adult worm dies in the peritoneum.4
Migration of adult worms into the biliary tree can lead to biliary colic, pyogenic cholangitis, cholecystitis, empyema of the gallbladder, hepatic abscess, septicemia, cholelithiasis, stricture formation, and pancreatitis.3,4,9 Rarely, ascariasis can lead to aseptic encephalopathy.10
Chronic A lumbricoides infection can lead to nutritional deficiencies. Children with chronic ascariasis typically have lower levels of serum hemoglobin, ferritin, retinol, and albumin.11,12 Chronic ascariasis is associated with impaired physical growth and intellectual development, particularly in growing children.13,14
DIFFERENTIAL DIAGNOSIS
Other soil-transmitted helminths that may be excreted are the whipworm (Trichuris trichiura) and hookworms (Necator americanus and Ancylostoma duodenale).5
DIAGNOSTIC STUDIES
Diagnosis of A lumbricoides infection is best established by microscopic examination of fecal smears for characteristic ova; larvae may also be detected in the sputum.1 If a worm is excreted, pathological examination yields a definitive diagnosis-as was the case in this patient.
Imaging is usually reserved for more severe cases. A chest radiograph or CT scan will display ground-glass opacity in Ascaris pneumonia.8 The roundworms usually are not visible on plain abdominal radiographs unless barium contrast is used.8 CT and ultrasonography can help in detecting the worms in both the intestines and biliary system.3,8 Endoscopic retrograde cholangiopancreatography is useful in visualizing the exact location of roundworms in the biliary system and is usually done in cases in which endoscopic removal of the worm is indicated.8 Magnetic resonance cholangiopancreatography is a less invasive alternative for pinpointing the worm location.8
TREATMENT
Benzimidazoles, such as mebendazole (100 mg PO bid for 3 days or 500 mg PO once) and albendazole (400 mg PO once), are effective treatments of intestinal ascariasis in patients of all ages.6 Pyrantel pamoate (11 mg/kg PO once, maximum 1 g) is a suitable alternative.6
Surgery may be required for intestinal obstruction. Endoscopic or laparoscopic removal of the worms may be indicated in patients with severe intestinal and biliary system complications.1,4
In regions where the prevalence of ascariasis is greater than 50%, prophylactic treatment with deworming agents for school-aged children can help control the spread of the disease.6 Improved sanitary conditions, proper disposal of human excreta, and discontinuing the use of human fecal matter as a fertilizer are effective long-term preventive measures.15
References:
REFERENCES:
1. Khuroo MS. Ascariasis. Gastroenterol Clin North Am. 1996;25:553-577.
2. Ugbomoiko US, Dalumo V, Ofoezie IE, Obiezue RN. Socio-environmental factors and ascariasis infection among school-aged children in Ilobu, Osun State, Nigeria. Trans R Soc Trop Med Hyg. 2009;103:223-228.
3. Shah OJ, Zargar SA, Robbani I. Biliary ascariasis: a review. World J Surg. 2006;30:1500-1506.
4. Bethony J, Brooker S, Albonico M, et al. Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet. 2006;367:1521-1532.
5. Nchito M, Geissler PW, Mubila L, et al. The effect of iron and multi-micronutrient supplementation on Ascaris lumbricoides reinfection among Zambian schoolchildren. Trans R Soc Trop Med Hyg. 2009;103:229-236.
6. Dent AE, Kazura JW. Ascariasis (Ascaris lumbricoides). In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia: Saunders Elsevier, 2007:1495-1496.
7. Gangopadhyay AN, Upadhyaya VD, Gupta DK, et al. Conservative treatment for round worm intestinal obstruction. Indian J Pediatr. 2007;74:1085-1087.
8. Park MS, Kim KW, Ha HK, Lee DH. Intestinal parasitic infection. Abdom Imaging. 2008;33:166-171.
9. Das CJ, Kumar J, Debnath J, Chaudhry A. Imaging of ascariasis. Australas Radiol. 2007;51:500-506.
10. Jat KR, Marwaha RK, Panigrahi I, Gupta K. Ascariasis-associated worm encephalopathy in a young child. Trop Doct. 2009;39:113-114.
11. Wani SA, Ahmad F, Zargar SA, et al. Soil-transmitted helminths in relation to hemoglobin status among school children of the Kashmir Valley. J Parasitol. 2008;94:591-593.
12. Al-Mekhlafi MH, Azlin M, Aini UN, et al. Prevalence and predictors of low serum retinol and hypoalbuminaemia among children in rural Peninsular Malaysia. Trans R Soc Trop Med Hyg. 2007;101:1233-1240.
13. Jardim-Botelho A, Raff S, Rodrigues Rde A, et al. Hookworm, Ascaris lumbricoides infection and polyparasitism associated with poor cognitive performance in Brazilian schoolchildren. Trop Med Int Health. 2008;13:994-1004.
14. Holland CV. Predisposition to ascariasis: patterns, mechanisms and implications. Parasitology. 2009;136:1537-1547.
15. Kurosawa CM, Ito T, Takaki J, et al. The half-life of Ascaris lumbricoides prevalence in Japanese schoolchildren. Acta Med Okayama. 2008;62:303-312.






















