Influenza and RSV: How to suspect, diagnose, treat
Respiratory syncytial virus (RSV) and Influenza are responsible for significant morbidity and mortality in children. Pediatricians must step up vigilance to ensure early diagnosis and treatment.

")
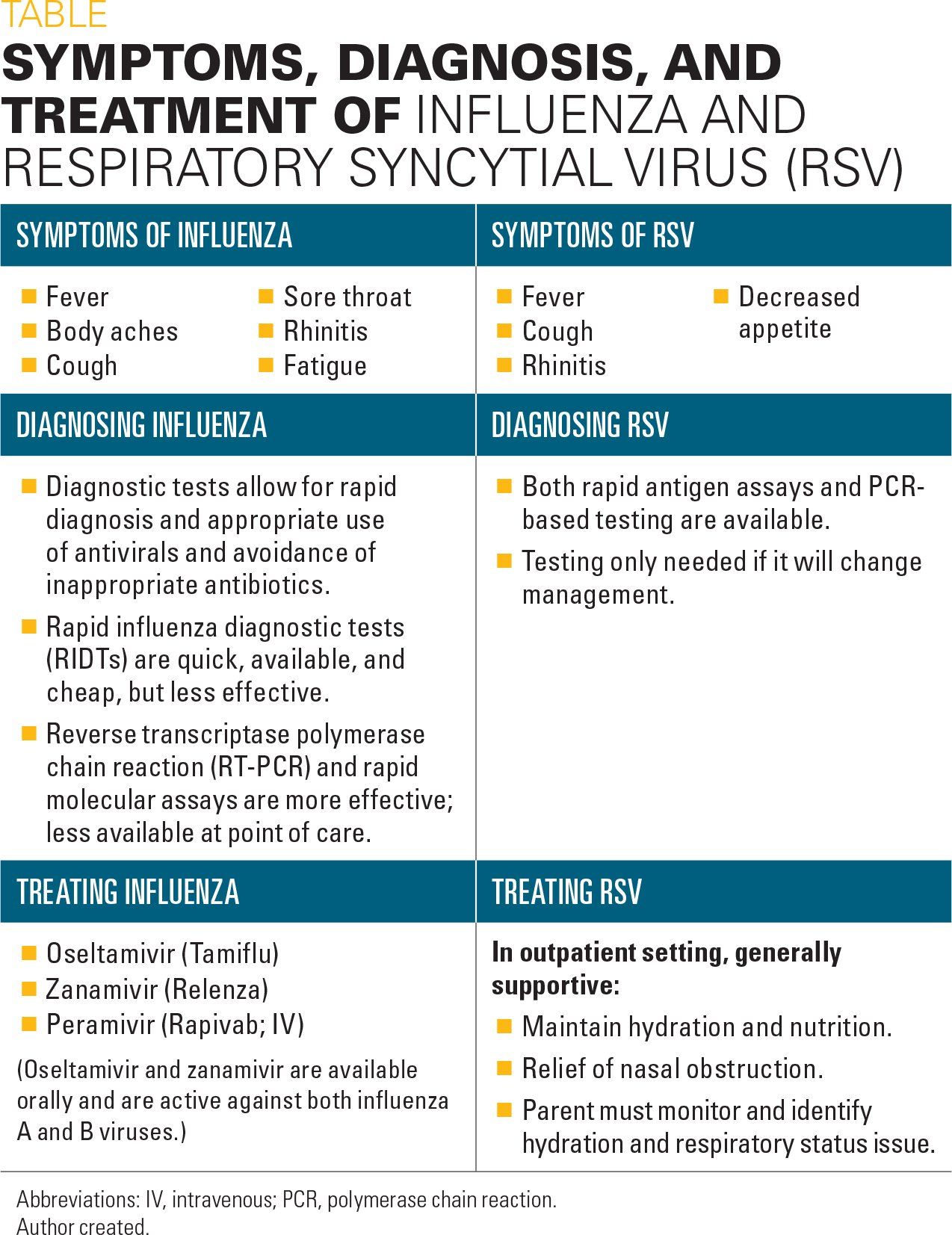
Table
Influenza and respiratory syncytial virus (RSV) represent a significant amount of the disease burden a pediatrician sees in the winter months. Both diseases lead to considerable morbidity and mortality in the pediatric population. This article reviews the impacts of these diseases on children and what the pediatrician in the trenches needs to know about diagnosis and treatment.
Influenza
Although the symptoms of influenza (Table) peak between December and March, cases are seen from October through May.1
The clinician should suspect influenza regardless of immunization status during influenza season among all febrile pediatric patients, but especially among febrile infants and children with:2,3
· Rapid onset of acute respiratory illness with fever.
· An exacerbation of chronic respiratory disease with fever.
· Fever, cough, and sore throat and no other cause during flu season.
· Community-acquired pneumonia.
Typical symptoms include:4
· Sudden onset of fever.
· Headache.
· Myalgia.
· Malaise.
· Respiratory symptoms such as upper respiratory infection (URI), cough, or sore throat.
However, children aged younger than 2 months may have a sepsis-like presentation, and the immunocompromised may be afebrile and lack systemic symptoms.
Children tend to shed virus longer compared with adults before (2-3 days vs 1 day, respectively) and after (7-10 days vs 4-5 days, respectively) the onset of symptoms.5
Diagnosis of influenza
Given the common symptoms, the pediatrician might then assume that making an influenza diagnosis is relatively straightforward and easy. However, in one outbreak of influenza, other viruses leading to a “flu-like” illness (rhinovirus, parainfluenza, and human metapneumovirus) were more common and clinical presentation for each was similar.6 Appropriate diagnosis allows for optimization in antiviral treatment and decreased use of inappropriate antibiotics and other testing. Rapid diagnosis also may improve satisfaction with the healthcare provider.
Depending on the testing modality used in the office or emergency department (ED), an influenza diagnosis is dependent on either identification of virus or the detection of viral protein/viral RNA in respiratory tract secretions.7 Negative antigen tests do not rule out an influenza infection.
Rapid influenza diagnostic tests (RIDTs) utilizing viral antigen detection are commonly performed in the outpatient setting because results are obtained quickly, usually before the end of the visit. However, these tests have a lower sensitivity (50%-70%) than other currently available tests.7 Reverse transcriptase polymerase chain reaction (RT-PCR) and rapid molecular assays are 2 other testing modalities with improved sensitivity (86%-100% and 66%-100%, respectively) and are available as Clinical Laboratory Improvement Amendments (CLIA)-waived tests that can be used at point of care.8
Impact of influenza in pediatric patients
Approximately 9% of all children experience a symptomatic influenza infection yearly that is associated with increased physician visits, increased antibiotic use, and missed time from work and school.9-11 The majority of hospitalizations in influenza-confirmed pediatric patients occur in either patients with no known high-risk condition, a chronic lung condition, or a neurologic condition.12
How effective is influenza vaccination?
Effectiveness of the influenza vaccine is determined by the fit or match between the influenza strains in the vaccine and the particular viruses actually circulating during influenza season as well as their severity.13-16 When the fit is high, good rates of protection are seen, and vice versa.
Vaccine effectiveness measures how well vaccination prevents influenza infection in a routine community setting. Over the 14 flu seasons from 2004 to 2018, the estimated influenza vaccination effectiveness ranged from 10% to 60% with effectiveness greater than 40% 9 times.17
Although uncommon, influenza is associated with more than 100 deaths annually among children and adolescents, ranging from 37 in the 2011-2012 flu season to 358 in the 2009 pandemic.18
Examining laboratory-confirmed flu deaths over 4 flu seasons from 2010 to 2014, Flannery and colleagues18 found that only 26% received flu vaccination 14 days before symptom onset. The vaccination rate among children with high-risk conditions related to flu was only slightly better at 31%.
Overall vaccine effectiveness was 51% and 65%, respectively, for children with and without high-risk conditions. These results indicate the continued need for the pediatrician to increase vaccination rates, especially for those children with high-risk conditions.18
Influenza treatment
Oseltamivir (Tamiflu), zanamivir (Relenza), and peramivir (Rapivab) are neuraminidase inhibitors that are currently available in the United States. Oseltamivir and zanamivir are available orally and are active against both influenza A and B viruses. Peramivir is an intravenous (IV) formulation and indicated in patients aged older than 2 years with symptoms for fewer than 2 days.
A neuraminidase inhibitor was recommended as the treatment of choice during the 2017-2018 flu season as more than 99% of circulating viruses were susceptible.19
Amantadine and rimantadine are adamantanes and were not recommended for the treatment or prophylaxis of influenza during the 2017-2018 season.19
The Centers for Disease Control and Prevention (CDC) provides frequent updates for prophylaxis and treatment based on circulating strains and resistance patterns, available at www.cdc.gov/flu/professionals/antivirals/index.htm.
Treatment with a neuramidase inhibitor decreases symptom duration by approximately 1 day, decreases associated otitis media, and decreases prescription of unnecessary antibiotics.20,21 Additionally, earlier treatment (eg, 12-24 hours after symptoms onset) can significantly decrease symptom duration.22,23 In 1 study of children aged 1 to 3 years, treatment within 24 hours with oseltamivir decreased symptom duration by 3 days.23
Finally, among patients admitted to intensive care units, early treatment was associated with increased survival.24 Year-round vaccination of pregnant women in a study in Nepal decreased maternal febrile flu-like illnesses by 19%, infants aged younger than 6 months diagnosed with flu by 30%, and low-birth-weight by 15%.25
Respiratory syncytial virus
Globally, RSV is second only to malaria as a cause of death from infectious agents in children aged from 28 to 364 days.26 In the United States, the RSV-associated pneumonia mortality rate is 3.1 per 100,000 person-years in children aged 1 year.27,28 These RSV infections additionally result in significant morbidity among pediatric patients.
Symptoms of RSV
Symptoms (Table) depend on the age of the child and his/her underlying health status. Infants and young children are more likely to present with bronchiolitis or pneumonia whereas older children are more likely to present with upper respiratory tract symptoms.29,30 Of note, RSV infection also may present as apnea, and some authors have discussed an association with sudden infant death syndrome.31,32
Diagnosing RSV
Respiratory syncytial virus is commonly diagnosed clinically when a young child presents with lower respiratory disease in the winter months with RSV circulating in the community. A laboratory diagnosis is often pursued when it will impact the clinical management.
Both rapid antigen assays and PCR-based diagnostic technologies are available when necessary.
Treating RSV
Respiratory syncytial virus that is not severe can generally be managed in the outpatient setting with supportive care.
Supportive measures include:
· Adequate ability to maintain hydration and nutrition.
· Relief of nasal obstruction.
· Ability of parent to monitor and identify hydration and respiratory status.
Neither oral nor inhaled bronchodilators are recommended in the routine outpatient treatment of RSV as they do not decrease any long-term outcomes.33-35 Similarly, neither treatment with steroids nor montelukast decreased respiratory or wheezing symptoms following RSV infection.36,37 Antibiotics are only indicated if there is a coexisting bacterial infection.38
Follow-up either by phone or in person should occur in 1 to 2 days depending on how severe the child is at presentation.
When to hospitalize
Indications for hospital admission include:
· Dehydration.
· Toxic appearance.
· Lethargy.
· Signs of respiratory distress such as inability to feed, nasal flaring, retractions, or a respiratory rate greater than 70 breaths per minute.
· Apnea.
· Hypoxia.
· Concern about parent’s ability to care for child.
For children requiring hospital admission, supportive care remains the standard treatment. Admitted children should be placed on contact precautions and monitored closely for hydration status.
Rapid respiratory rate and moderate-to-severe respiratory distress are possible indications for parenteral-only fluid administration to avoid any risk of aspiration. Urine output needs to be monitored closely.
Respiratory support is the mainstay of treatment. Oxygen should be administered if SpO2 is 90% or lower to maintain an SpO2 above 90% to 92%.38,39 Chest physiotherapy is not routinely recommended but may be beneficial in patients with some diseases such as cystic fibrosis.40
Bronchodilators are not routinely recommended.38 Similarly, neither systemic nor inhaled glucocorticoids have been found to prevent admission, decrease length of stay, decrease objective measurements of severity in patients with more severe disease, or readmission among patients with a first episode of bronchiolitis.37
Although a 2009 study did find that combining systematic glucocorticoids and bronchodilators may decrease hospitalization rates, the result was not considered statistically significant when adjusted for multiple comparisons. Additional study is necessary before this treatment approach can be recommended.41,42
The administration of hypertonic saline has had mixed results in the literature with some studies showing positive effects and others having negative results. A 2013 Cochrane Review concluded that hypertonic saline decreased length of stay and decreased symptoms, but also cautioned that more research was necessary to evaluate its effectiveness.43 More recent, well-designed, randomized controlled trials have not shown a benefit related to outcomes such as severity scores, length of stay, readiness for discharge, or subsequent readmission rates.44-46 The 2014 guidelines from the American Academy of Pediatrics (AAP) do not recommend treatment with nebulized hypertonic saline in the ED, but do find relatively weak evidence to support treatment in hospitalized patients.38
Looking ahead
On the research front, lumicitabine is a nucleoside analog that was shown to reduce RSV viral load and symptoms among healthy volunteers. Participants treated with the study drug cleared virus more than 80% faster than those treated with placebo and also had improved clinical status.47 Several different clinical trials with this study drug are currently in progress with infants and young children.
In terms of prevention, handwashing, avoiding persons with URIs, and avoiding cigarette smoke remain routine recommendations for the pediatrician. Immunoprophylaxis with the monoclonal antibody palivizumab is recommended for certain preterm infants, infants with chronic lung disease, and infants with hemodynamically significant congenital heart disease in the first year of life.48,49
Following the most recent update of the RSV guidelines in 2014, which stated that palivizumab was not of high value because of its high cost and minimal benefit, significantly fewer infants qualified for treatment. Rajah and colleagues found that in the year following the AAP recommendation, there was a significant increase in RSV hospitalizations and associated morbidity such as increased lengths of stay, hospital costs, admissions to intensive care units (ICUs), and oxygen requirements compared with the previous year.50 However, pooling data from 8 Medicaid health plans in Texas, Farber was not able to demonstrate similar outcomes.51
Although there is not currently an RSV vaccine, there are as many as 10 vaccines and 11 novel clinical therapeutic agents in development.52 These include therapies that provide anti-RSV neutralizing antibodies as well as monoclonal antibodies targeting the RSV protein structure.
Summary
Respiratory syncytial virus and Influenza are responsible for significant morbidity and mortality in the pediatric population. Continued vigilance for immunizing against influenza and early diagnosis and treatment are important for the pediatrician. Whereas current prevention and treatment options for RSV are suboptimal, a number of investigational therapies are on the horizon.
References:
1. Centers for Disease Control and Prevention. The flu season. Available at: https://www.cdc.gov/flu/about/season/flu-season.htm. Updated July 12, 2018. Accessed August 28, 2018.
2. Möst J, Weiss G. Consecutive infections with influenza A and B virus in children during the 2014-2015 seasonal influenza epidemic. J Infect Dis. 2016;214(8):1139-1141.
3. Harper SA, Bradley JS, Englund JA, et al; Expert Panel of the Infectious Diseases Society of America. Seasonal influenza in adults and children-diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2009;48(8):1003-1032.
4. Silvennoinen H, Peltola V, Lehtinen P, Vainionpää R, Heikkinen T. Clinical presentation of influenza in unselected children treated as outpatients. Pediatr Infect Dis J. 2009;28(5):372-375.
5. Harper SA, Fukuda K, Uyeki TM, et al; Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP). Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2004;53(RR-6):1-40.
6. Chang ML, Jordan-Villegas A, Evans A, et al. Respiratory viruses identified in an urban children’s hospital emergency department during the 2009 influenza A(H1N1) pandemic. Pediatr Emerg Care. 2012;28(10):990-997.
7. Merckx J, Wali R, Schiller I, et al. Diagnostic accuracy of novel and traditional rapid tests for influenza infection compared with reverse transcriptase polymerase chain reaction: a systematic review and meta-analysis. Ann Intern Med. 2017;167(6):394-409.
8. Centers for Disease Control and Prevention. Information on rapid molecular as-says, RT-PCR, and other molecular assays for diagnosis of influenza virus infection. Available at: https://www.cdc.gov/flu/professionals/diagnosis/molecular-assays.htm. Updated February 20, 2018. Accessed August 28, 2018.
9. McLean HQ, Peterson SH, King JP, Meece JK, Belongia EA. School absenteeism among school-aged children with medically attended acute viral respiratory ill-ness during three influenza seasons, 2012-2013 through 2014-2015. Influenza Other Respir Viruses. 2017;11(3):220-229.
10. Petrie JG, Cheng C, Malosh RE, et al. Illness severity and work productivity loss among working adults with medically attended acute respiratory illnesses: US Influenza Vaccine Effectiveness Network 2012-2013. Clin Infect Dis. 2016;62(4):448-455.
11. Tokars JI, Olsen SJ, Reed C. Seasonal incidence of symptomatic influenza in the United States. Clin Infect Dis. 2018;66(10):1511-1518.
12. Centers for Disease Control and Prevention. Weekly U.S. Influenza Surveil-lance Report. 2017-2018 influenza season week 33 ending August 18, 2018. Available at: https://www.cdc.gov/flu/weekly/index.htm. Updated August 24, 2018. Accessed August 28, 2018.
13. Belshe RB, Coelingh K, Ambrose CS, Woo JC, Wu X. Efficacy of live attenuated influenza vaccine in children against influenza B viruses by lineage and antigenic similarity. Vaccine. 2010;28(9):2149-2156.
14. Giezeman KM, Nauta J, de Bruijn IA, Palache AM. Trivalent inactivated subunit influenza vaccine Influvac: 25-year experience of safety and immunogenicity. Vaccine. 2009;27(18):2414-2417.
15. Osterholm MT, Kelley NS, Sommer A, Belongia EA. Efficacy and effectiveness of influenza vaccines: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(1):36-44.
16. Jain VK, Rivera L, Zaman K, et al. Vaccine for prevention of mild and moderate-to-severe influenza in children. N Engl J Med. 2013;369(26):2481-2491.
17. Centers for Disease Control and Prevention. Seasonal influenza vaccine effectiveness, 2005-2018. Available at: https://www.cdc.gov/flu/professionals/vaccination/effectiveness-studies.htm. Updated February 15, 2018. Accessed August 28, 2018.
18. Flannery B, Reynolds SB, Blanton L, et al. Influenza vaccine effectiveness against pediatric deaths: 2010-2014. Pediatrics. 2017;139(5):e20164244.
19. Budd AP, Wentworth DE, Blanton L, et al. Update: Influenza activity-United States, October 1, 2017-February 3, 2018. MMWR Morb Mortal Wkly Rep. 2018;67(6):169-179.
20. Jefferson T, Jones M, Doshi P, Spencer EA, Onakpoya I, Heneghan CJ. Oseltamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ. 2014;348:g2545.
21. Whitley RJ, Hayden FG, Reisinger KS, et al. Oral oseltamivir treatment of influenza in children. Pediatr Infect Dis J. 2001;20(2):127-133.
22. Kawai N, Ikematsu H, Iwaki N, et al. Factors influencing the effectiveness of oseltamivir and amantadine for the treatment of influenza: a multicenter study from Japan of the 2002-2003 influenza season. Clin Infect Dis. 2005;40(9):1309-1316.
23. Heinonen S, Silvennoinen H, Lehtinen P, et al. Early oseltamivir treatment of influenza in children 1-3 years of age: a randomized controlled trial. Clin Infect Dis. 2010;51(8):887-894.
24. Louie JK, Yang S, Samuel MC, Uyeki TM, Schechter R. Neuraminidase inhibitors for critically ill children with influenza. Pediatrics. 2013;132(6):e1539-e1545.
25. Steinhoff MC, Katz J, Englund JA, et al. Year-round influenza immunisation during pregnancy in Nepal: a phase 4, randomised, placebo-controlled trial. Lancet Infect Dis. 2017;17(9):981-989.
26. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-2128.
27. Byington CL, Wilkes J, Korgenski K, Sheng X. Respiratory syncytial virus-associated mortality in hospitalized infants and young children. Pediatrics. 2015;135(1):e24-e31.
28. Geoghegan S, Erviti A, Caballero MT, et al. Mortality due to respiratory syncytial virus. Burden and risk factors. Am J Respir Crit Care Med. 2017;195(1):96-103.
29. Hall CB, Long CE, Schnabel KC. Respiratory syncytial virus infections in previously healthy working adults. Clin Infect Dis. 2001;33(6):792-796.
30. Glezen WP, Taber LH, Frank AL, Kasel JA. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child. 1986;140(6):543-546.
31. Uren EC, Williams AL, Jack I, Rees JW. Association of respiratory virus infections with sudden infant death syndrome. Med J Aust. 1980;1(9):417-419.
32. Ralston S, Hill V. Incidence of apnea in infants hospitalized with respiratory syncytial virus bronchiolitis: a systematic review. J Pediatr. 2009;155(5):728-733.
33. Patel H, Gouin S, Platt RW. Randomized, double-blind, placebo-controlled trial of oral albuterol in infants with mild-to-moderate acute viral bronchiolitis. J Pediatr. 2003;142(5):509-514.
34. Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;(6):CD001266.
35. Hartling L, Bialy LM, Vandermeer B, et al. Epinephrine for bronchiolitis. Cochrane Database Syst Rev. 2011;(6):CD003123.
36. Bisgaard H, Flores-Nunez A, Goh A, et al. Study of montelukast for the treatment of respiratory symptoms of post-respiratory syncytial virus bronchiolitis in children. Am J Respir Crit Care Med. 2008;178(8):854-860.
37. Fernandes RM, Bialy LM, Vandermeer B, et al. Glucocorticoids for acute viral bronchiolitis in infants and young children. Cochrane Database Syst Rev. 2013;(6):CD004878.
38. Ralston SL, Lieberthal AS, Meissner HC, et al; American Academy of Pediatrics. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474-e1502.
39. Panitch HB. Respiratory syncytial virus bronchiolitis: supportive care and therapies designed to overcome airway obstruction. Pediatr Infect Dis J. 2003;22(2 suppl):S83–S87.
40. Roqué i Figuls M, Giné-Garriga M, Granados Rugeles C, Perrotta C. Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database Syst Rev. 2012;(2):CD004873.
41. Frey U, von Mutius E. The challenge of managing wheezing in infants. N Engl J Med. 2009;360(20):2130-2133.
42. Plint AC, Johnson DW, Patel H, et al; Pediatric Emergency Research Canada (PERC). Epinephrine and dexamethasone in children with bronchiolitis. N Engl J Med. 2009;360(20):2079-2089.
43. Zhang L, Mendoza-Sassi RA, Wainwright C, Klassen TP. Nebulised hypertonic saline solution for acute bronchiolitis in infants. Cochrane Database Syst Rev. 2013;(7):CD006458.
44. Jacobs JD, Foster M, Wan J, Pershad J. 7% hypertonic saline in acute bronchiolitis: a randomized controlled trial. Pediatrics. 2014;133(1):e8-e13.
45. Everard ML, Hind D, Ugonna K, et al. Saline in acute bronchiolitis RCT and economic evaluation: hypertonic saline in acute bronchiolitis-randomized controlled trial and systematic review. Health Technol Assess. 2015;19(66):1-130.
46. Silver AH, Esteban-Cruciani N, Azzarone G, et al. 3% hypertonic saline versus normal saline in inpatient bronchiolitis: a randomized controlled trial. Pediatrics. 2015;136(6):1036-1043.
47. DeVincenzo JP, McClure MW, Symons JA, et al. Activity of oral ALS-008176 in a respiratory syncytial virus challenge study. N Engl J Med. 2015;373(21):2048-2058.
48. American Academy of Pediatrics Committee on Infectious Diseases; American Academy of Pediatrics Bronchiolitis Guidelines Committee. Policy statement: Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics. 2014;134(2):415-420. Erratum in: Pediatrics. 2014;134(6):1221.
49. American Academy of Pediatrics Committee on Infectious Diseases; American Academy of Pediatrics Bronchiolitis Guidelines Committee. Technical report: Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics. 2014;134(2):e620-e638.
50. Rajah B, Sánchez PJ, Garcia-Maurino C, Leber A, Ramilo O, Mejias A. Impact of the updated guidance for palivizumab prophylaxis against respiratory syncytial virus infection: a single center experience. J Pediatr. 2017;181:183.e1–188.e1.
51. Farber HJ. Impact of the 2014 American Academy of Pediatrics guidance on respiratory syncytial virus and bronchiolitis hospitalization rates for infants born prematurely. J Pediatr. 2017;185:250.
52. Mazur NI, Martinón-Torres F, Baraldi E, et al; Respiratory Syncytial Virus Net-work (ReSViNET). Lower respiratory tract infection caused by respiratory syncytial virus: current management and new therapeutics. Lancet Respir Med. 2015;3(11):888-900.