





Unexpected Finding in Young Girl After Arm Injury
A 10-year-old girl had pain in her left arm after falling off a bunk bed 4 days earlier. She denied fevers or other trauma. Since the fall, she had had difficulty in bearing weight on the arm. Her medical and family histories were unremarkable.





How Do You Read These Images?
A 10-year-old girl had pain in her left arm after falling off a bunk bed 4 days earlier. She denied fevers or other trauma. Since the fall, she had had difficulty in bearing weight on the arm. Her medical and family histories were unremarkable.
Examination revealed tenderness of the proximal left arm. Neurovascular findings were normal. No lymphadenopathy was appreciated.
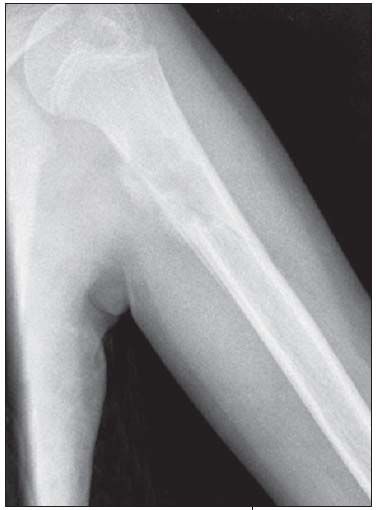
Anteroposterior and lateral views of the patient's left humerus were ordered.
What do these radiographs show?
A. Aneurysmal bone cyst.
B. Osteomyelitis.
C. Malignant lytic lesion.
D. Other.
Answer: D is the correct choice.



The radiographs show a centrally placed lytic lesion with lobulated contours and a well-defined transition zone in the proximal shaft of the humerus. An oblique pathological fracture runs through the cyst No other lesions are visible. A thick periosteal reaction on the medial aspect of the lytic lesion is also present; the periosteal reaction is atypical in this case; however, the radiographs were obtained 10 days after the fall.
This is a unicameral, or simple, bone cyst. Many of the lesions in the differential diagnosis, including aneurysmal bone cyst, osteomyelitis, malignant lytic lesion (such as eosinophilic granuloma or bone metastasis), can be excluded on the basis of location. The location of simple bone cysts is usually the humeral head, ball of the foot, proximal femur, or proximal humerus or calcaneus.
A simple bone cyst may be an incidental finding. However, like this child, most patients present with a pathological fracture. The pathognomonic sign after a fracture is a fallen fragment in the most dependent portion of the cyst. Occasionally, a periosteal reaction can be seen. A simple bone cyst is a fluid-filled cavity lined with fibrous tissue. It is thought to result from venous outflow obstruction, which leads to an increased intraosseous pressure and a consequent stimulation of
osteoclastic activity. This benign lesion usually devel-ops within the first 2 decades of life. The cyst causes bone instability and sometimes may be associated with pathological fractures after relatively minor trauma.
Simple bone cysts are usually asymptomatic and require observation only. Serial radiographs to monitor for continued bone destruction is needed only for large cysts with precarious cortical thinning. Physical activity is restricted to prevent fractures. Treatment of symptomatic cysts or cysts with impending fractures ranges from aspiration to resection, curettage, and bone grafting. The goal of treatment is a healed bone that is able to withstand the stress of physical activity-it is not radiographic resolution of the lesion. Success of treatment, regardless of the modality used, is age-related. Children older than 10 years have better results than those younger than 10 years. The cysts frequently recur in younger children and become stable at the onset of puberty. Spontaneous healing of the cyst with a fracture after closed fracture care has been reported.
This patient was treated with splint and cast for the fracture only.
















Recognize & Refer: Hemangiomas in pediatrics
July 17th 2019Contemporary Pediatrics sits down exclusively with Sheila Fallon Friedlander, MD, a professor dermatology and pediatrics, to discuss the one key condition for which she believes community pediatricians should be especially aware-hemangiomas.





