





Vesicoureteral Reflux
During hospitalization of a 6-month-old boy for respiratory syncytial virus infection, spiking fevers led to a bacteremia workup.


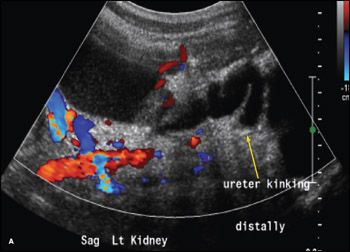
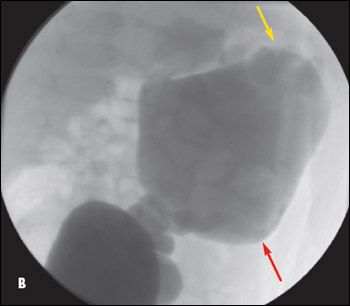
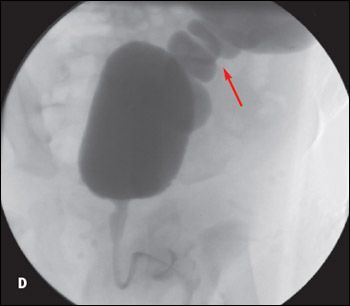
During hospitalization of a 6-month-old boy for respiratory syncytial virus infection, spiking fevers led to a bacteremia workup. This revealed Klebsiella species in his urine. A subsequent renal sonogram showed left-sided hydronephrosis, with a dilated, kinking, and tortuous ureter (A). The infant was given antibiotic prophylaxis and was scheduled for a voiding cystourethrogram as an outpatient. Results of this study showed a grade IV to V vesicoureteral reflux with distended renal pelvis (B, red arrow) significantly larger than the bladder (C, red arrow), thin renal parenchyma (B, yellow arrow), and tortuous left ureter (D, red arrow).
The infant had been born at full term via cesarean delivery because of breech presentation. Prenatal sonogram had shown duplication of the left collecting system. Immediately after birth, a urinary tract infection (UTI) developed, and the infant spent 2 weeks in the neonatal ICU. At 2 months of age, he had a second UTI, which was treated without follow-up. The mother reported that her infant sometimes passed urine that was puslike. Family history was unremarkable.


Examination revealed a palpable left kidney, tenderness in the left flank on palpation, and flank dullness. The abdomen was soft and nontender. A firm mass was noted on the left flank with questionable ballottability. The infant was readmitted for nephrostomy tube placement. His hospital course was uneventful.
Vesicoureteral reflux is the retrograde passage of urine from the bladder into the upper urinary tract. The primary type of vesicoureteral reflux is more common and results from congenital shortening of the intravesical portion of the ureter. Secondary vesicoureteral reflux is typically caused by a blockage in the urinary tract that results from anatomical abnormalities or UTIs. In children with febrile UTI, the risk of vesicoureteral reflux is increased. The condition is estimated to affect about 1% of newborns; it occurs twice as often in girls as in boys and is more likely to occur in infants and children younger than 2 years than in older children.1


Vesicoureteral reflux is classified into 5 grades. Spontaneous resolution generally occurs by age 5 years in 80% of patients with grade I or II reflux. In patients with grade III reflux, resolution is dependent on the age at presentation and the number of ureters involved; the resolution rate is higher in younger children (1 to 2 years) with unilateral disease and lower in older children (5 to 10 years) with bilateral reflux. In children with grade IV reflux (regardless of age at presentation), the resolution rate over 5 years is 60% for unilateral disease and less than 10% for bilateral reflux. In children with grade V reflux, spontaneous resolution rarely occurs without complications, the most common of which are renal scarring and secondary obstructive uropathy.2
Although the data on long-term outcomes are inconclusive, vesicoureteral reflux of any grade should be considered a risk factor for recurrent pyelonephritis and possible scarring.3

Treatment of grades I to III vesicoureteral reflux includes daily low-dose antibiotics (eg, trimethoprim/sulfamethoxazole, amoxicillin) until the reflux resolves or until the child is at least 5 years old. These patients require regular monitoring by a pediatric urologist to diagnose UTI and prevent the condition from worsening. Secondary reflux that does not resolve with antibiotic treatment, or that results in UTI despite antibiotic therapy (called breakthrough infections), and primary reflux that is severe (grades IV and V) require surgery to prevent permanent kidney damage.4
References:
REFERENCES:
1.
Hiraoka M, Hori C, Tsukahara H, et al. Vesicoureteral reflux in male and female neonates as detected by voiding ultrasonography.
Kidney Int
. 1999;55:1486-1490.
2.
Huang FY, Tsai TC. Resolution of vesicoureteral reflux during medical management in children.
Pediatr Nephrol
. 1995;9:715-717.
3.
Peru H, Bakkaloglu SA, Soylemezoglu O, et al. The relationship between urinary tract infections and vesicoureteral reflux in Turkish children.
Int Urol Nephrol
. 2009;41:947-951.
4.
Arant BS Jr. Vesicoureteral reflux and evidence-based management.
J Pediatr
. 2001;139:620-621.






















