





In Wheezing Infant With Toddler Sibling-Consider Foreign-Body Aspiration
I read with interest Drs Ha and Wilson’s “What’s Your Diagnosis?” case of an infant with a history of wheezing and dry cough ("History of Cough in an Infant and a Toddler"). In a setting such as this, one should also consider the possibility of foreign-body aspiration, which can result in recurring wheezing and pneumonia.


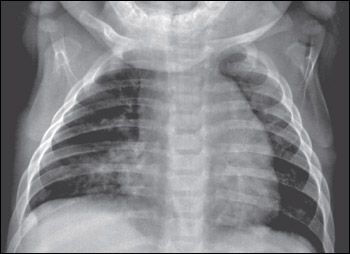
Figure – This infant's chest radiograph showed a right middle lobe infiltrate and peribronchial cuffing in both lung fields; these findings were consistent with the final diagnosis of recurrent respiratory illness manifesting as acute bronchiolitis and right middle lobe pneumonia.
I read with interest Drs Ha and Wilson's "What's Your Diagnosis?" case of an infant with a history of wheezing and dry cough ("History of Cough in an Infant and a Toddler") (Figure). In a setting such as this, one should also consider the possibility of foreign-body aspiration, which can result in recurring wheezing and pneumonia. The fact that this infant has a 2-year-old sister makes it quite possible that the toddler had shared food and other small objects with her younger brother, who at age 6 months would be developmentally capable of grasping his sister's offerings and putting them in his mouth. It's too bad a lateral chest radiograph was not available for assessment of this possibility.
We appreciate Dr Olufs' pertinent observation that foreignbody aspiration should be considered in infants and toddlers with a first presentation of reactive airway disease. This is particularly necessary when unilateral atelectasis is present-a finding that is best identified by assessing asymmetry on a lateral film, as Dr Olufs suggests. Although this infant's lateral radiograph was not pictured in the journal, it was available and did not suggest foreign-body aspiration. Nonetheless, follow-up consideration of this diagnosis is always necessary, because children who have aspirated a foreign object may show a transient response to bronchodilator therapy.






















