





Would you continue acne therapy for a teenage boy with severe scarring?
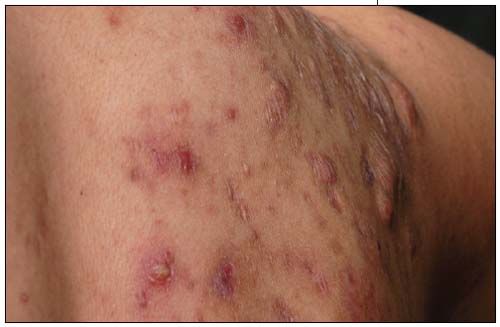
This 16-year-old boy has had severe nodulocystic acne that has responded to isotretinoin therapy. Unfortunately, this therapy was initiated after the scarring process-shown here on the back and shoulder-had developed.



Case:
This 16-year-old boy has had severe nodulocystic acne that has responded to isotretinoin therapy. Unfortunately, this therapy was initiated after the scarring process-shown here on the back and shoulder-had developed.
Is there any value in continuing the acne treatment? What advice can you offer the patient on the scarring?





(Answer and discussion on next page.)
Dermclinic–Answer
Yes, the primary treatment of the keloids in this patient is acne management; however, it must be stressed that the scars are permanent.
The term “keloid” is derived from the Greek word chele, which means crab claw. The crab claw is clearly evident on this boy's chest. A keloid former, such as this patient, probably has a genetic predisposition for this skin response. Keloids may affect all races and any site of the body. They are more common in dark-skinned children, in adolescence, and in certain areas (the anterior chest, shoulders, posterior neck, and earlobes). They usually develop after a skin injury, particularly thermal injury, or within wounds under tension. Keloids may also develop spontaneously, without a history of obvious injury or inflammation, particularly on the anterior chest.



It is useful to differentiate keloids from hypertrophic scars because the treatment and prognosis are quite different. Both types of scarring start as inflammatory lesions in the wound and usually produce an itching or burning sensation. The hypertrophic scar remains confined to the wound margin, whereas the keloid extends beyond the wound margin and often exhibits expanding, thick, inflammatory borders with central clearing; hence, the term “crab claw.” Hypertrophic scars tend to improve over time and respond quickly to intralesional corticosteroid therapy. Keloids are progressive and respond poorly to all forms of intervention.



The primary treatment of keloids is to stop the inflammatory insult. For this teenage boy, I chose to treat his acne with a second course of isotretinoin. Simultaneously, I began intralesional corticosteroid therapy with triamcinolone acetonide, at both 10 mg/mL and 40 mg/mL concentrations depending on the keloid density. The injection technique requires luer lock syringes; significant resistance during injection ensures placement of the corticosteroid in the keloid. For particularly dense keloids, I pretreat the lesion with cryosurgery to produce tissue swelling, which allows for easier penetration of the corticosteroid. I am also encouraging him to apply silicone gel both as sheeting and as a topical ointment. His treatment is likely to be a mutli-year project. I anticipate that he will be able to wear T-shirts without bumps showing through; however, he will always have the scars. I stress this to him at every visit to avoid creating unrealistic expectations of what I can do for him.
The medical literature reports a variety of other treatment options. Unfortunately, the trials are usually small and the results do not document the long-term success of the treatments. Pulsed dye laser, radiation, intralesional interferon, and intralesional 5-fluorouracil are the most common alternatives.
















Recognize & Refer: Hemangiomas in pediatrics
July 17th 2019Contemporary Pediatrics sits down exclusively with Sheila Fallon Friedlander, MD, a professor dermatology and pediatrics, to discuss the one key condition for which she believes community pediatricians should be especially aware-hemangiomas.





