





Parental postpartum depression: More than “baby blues”
Pediatricians need to recognize symptoms of perinatal depression in new mothers, provide basic counseling and treatment, and refer for appropriate services when needed.


Statistics regarding PPD



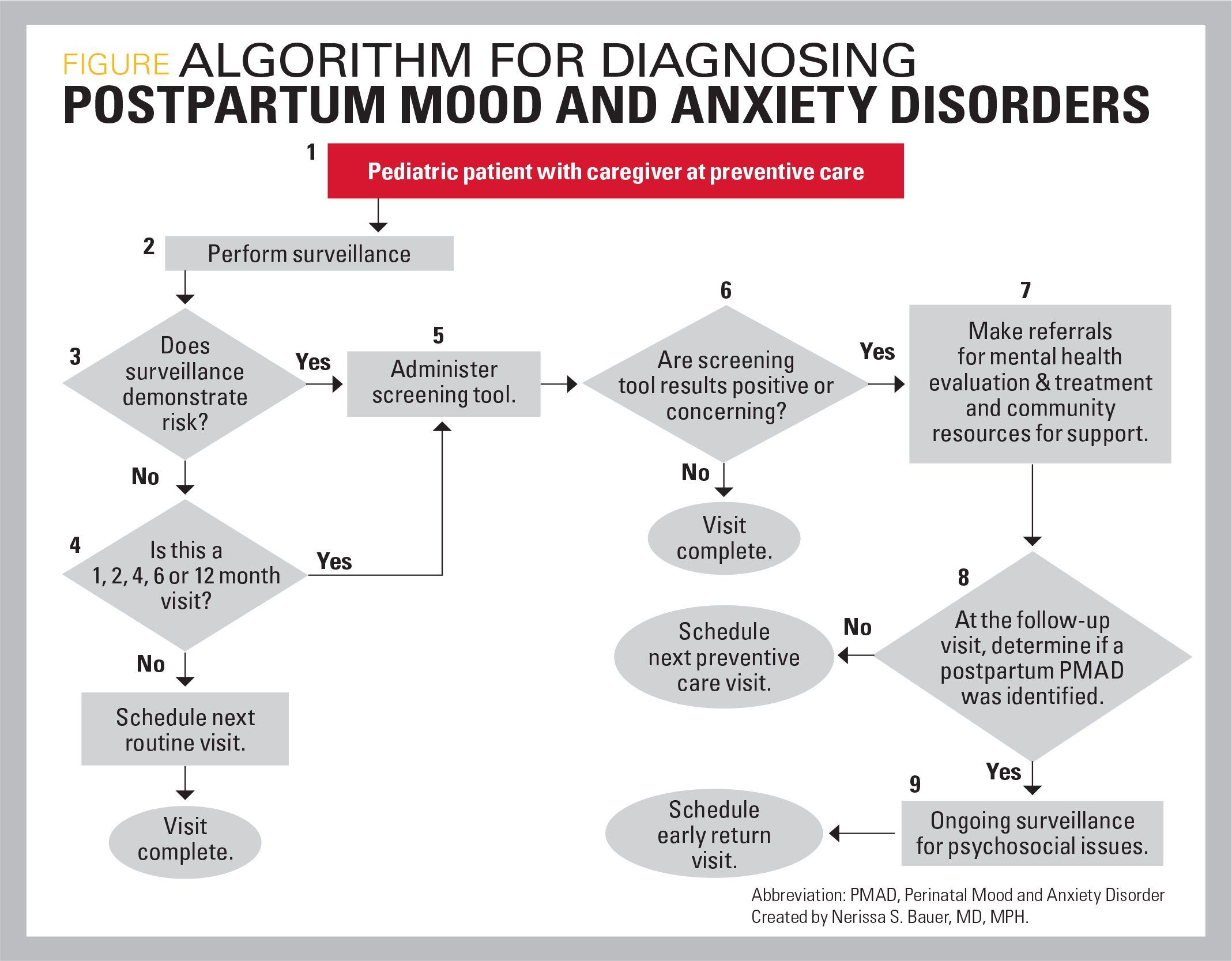
Algorithm for diagnosing postpartum mood and anxiety disorders
With more than 400,000 infants born to mothers who are depressed, perinatal depression is the most underdiagnosed obstetric complication in the United States.1 This article will review the spectrum of disease the pediatrician is likely to encounter, risk factors, and basic management when faced with this common problem.
Spectrum of postpartum depression
Postpartum depression (PPD) can be seen as a spectrum of disease across 3 main categories: 1) postpartum blues, 2) PPD, and 3) postpartum psychosis.1,2
Postpartum blues
Postpartum blues reportedly occurs in 50% to 80% of new mothers and occurs in the first few days after delivery. Symptoms typically resolve within a few days to 1 to 2 weeks following delivery. Postpartum blues do not impair maternal function and mothers can be treated with emotional support and reassurance.1,2
Symptoms of postpartum blues include:
· Anxiety
· Crying
· Decreased appetite
· Exhaustion
· Loss of interest in usual activities
· Mood swings
· Sadness
· Sleeping problems
· Worrying
Postpartum depression
Postpartum depression occurs in 13% to 20% of women following childbirth and meets the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for depression. It is distinct from postpartum blues in several ways. Symptoms occur beyond the first 2 weeks postpartum, peaking within the first 4 months following delivery, but PPD can occur anytime within the first year of the child’s life.1,2
Whereas the symptoms experienced may be similar to postpartum blues, the severity and duration of symptoms of PPD differentiate it from postpartum blues. Symptoms in PPD last longer than 2 weeks, occur almost daily, last throughout the day, and may result in functional impairment. Symptoms may persist for several months up to a year.1,2
Postpartum psychosis
Postpartum psychosis is an uncommon mental health emergency that puts both mother and child at risk. It typically occurs in the first month postpartum with mothers experiencing paranoia, hallucinations, delusions, and suicidal or homicidal thoughts. Bipolar disorder increases the risk, but it can occur in patients without a prior psychiatric history.2
Risk factors
The most significant risk factor for PPD is a history of depression-increasing the risk of PPD by a factor of 20. Other factors such as maternal age, pregnancy complications, and obstetric issues all potentially contribute. In relation to maternal age, both adolescent (relative risk [RR],1.48) and advanced maternal age (>35 years: RR, 1.25) mothers were at higher risk of PPD.3
Diabetes also increases risk, but gestational diabetes (RR, 1.7) surprisingly increased risks more than pregestational diabetes (RR, 1.32). Similarly, prematurity increased risks of PPD with earlier prematurity having an incremental impact (32 weeks’ gestation: RR, 1.36; and 32-36 weeks: RR, 1.2).3
Other possible risks include:
· Being single4
· Multiparous5
· Family history of PPD6
· History of prior abuse7
Impact of PPD
Maternal depression adversely impacts an infant's development and can decrease attachment and bonding. Infants living in a setting of maternal depression demonstrate less social interaction and suffer from delays in development. Failure to identify and treat maternal depression can lead to persisting attachment issues that are less likely to respond to intervention over time.1,2 Further, depression can lead to a neglectful environment that impacts early brain development and subsequent visible changes on magnetic resonance imaging of the brain.1
Maternal depression is associated with a number of cognitive and social-emotional aspects of development. A number of behaviors associated with language development (eg, reading to, speaking to, and cuddling with an infant) are less likely to occur with maternal depression. Infants of depressed mothers may look at the mother less often and show less engagement with their environment as early as age 2 months.1
Maternal depression is also associated with a number of negative practices and beliefs related to breastfeeding. Depression is associated with decreased mother-infant interactions that may lead to the mother failing to interpret her infant's cues and may result in the infant becoming fussy, withdrawn, or more likely to develop feeding or sleeping problems. This attachment issue can lead to failure to thrive, increased risk for accidents resulting from parental inattention, nonaccidental trauma, as well as increased sick visits and emergency department use.2
Although maternal depression has not been associated with decreased well-child visits, it seems to be associated with increases in the likelihood of parenting practices that are inconsistent with national guidelines and are associated with poorer health outcomes.1,2 Depressed mothers are less likely to integrate well-child advice from the pediatrician. Depressed mothers are less likely to place their infant on its back, more likely to put their child to bed with a bottle, and less likely to engage in other preventive healthcare pracctices.8,9 Other research has shown depressed mothers more likely to smoke, to appropriately administer vitamins, to use a car seat appropriately, to cover electrical plugs, or to have syrup of ipecac in the home.10,11
Long-term PPD may result in an increased risk of the infant developing behavioral issues and mood disorders as an adolescent or adult.2
Paternal PPD
Although not discussed as commonly as maternal PPD, paternal PPD occurs more commonly in the United States with a 14% prevalence rate. Paternal PPD is more likely to occur between 3 and 6 months postpartum, and risk factors include prior depression history, lower socioeconomic status, having other children, and maternal prenatal depression. Paternal PPD is similarly associated with behavioral and emotional problems later in childhood.2
Most pediatricians don't screen for PPD
Less than half of pediatricians ask mothers about depressive symptoms. Screening for PPD among pediatricians increased from 33% to 44% between 2004 and 2013 in periodic surveys performed by the American Academy of Pediatrics (AAP). The increase was felt to result from pediatricians’ responsibility for addressing social-emotional familial factors within their practice.12
There is a tremendous opportunity for pediatricians to address this disparity as mothers appear to be willing to discuss mental health issues at pediatric visits, so incorporating screening and treatment into busy pediatric practices is feasible.13,14
The AAP recommends screening for maternal depression at 1, 2, 4, and 6 months.1
There are a number of validated tools that can be used in the office to screen for PPD:
· Edinburgh Postnatal Depression Scale (EPDS)
· EPDS-3
· Patient Health Questionnaire (PHQ-9)
· PHQ-2
The EPDS is a 10-item questionnaire that asks about symptoms of emotional distress within the prior 7 days and takes less than 5 minutes to complete. The items are scored on a 4-point scale with a maximum score of 30. Scores of 10 or greater indicate a risk for depression is present. Additionally, item 10 is a suicidality indicator and indicates a positive screen if answered affirmatively. Scores of 10 or greater should be repeated in 2 weeks, and 2 scores above 12 indicate a need for further intervention.15
A shortened version of the EPDS uses 3 items from the anxiety subscale that can be used to identify patients who need to complete the entire instrument. The EPDS-3 identifies symptoms of self-blame, feeling panicky, and being anxious or worried for no good reason. Scores are multiplied by 10 and divided by 3. Scores of greater than or equal to 10 are considered positive. The sensitivity for the instrument is 0.95 and the specificity is .80. The positive and negative predictive values were .56 and .98, respectively.16
The PHQ-9 and PHQ-2 are not specific for PPD but are validated instruments for identifying depression in the primary care setting. The PHQ-9 asks about symptoms over a 2-week period that are rated on a 4-point scale. Scores grade symptoms as mild (10-14), moderate (14-19), or severe (20+).17 The PHQ-2 asks about frequency of depressed mood and anhedonia over a 2-week period that is also assessed on a 4-point scale.18 Many organizations utilize a stepped approach with patients who answer 1 of the 2 items positively rather than complete the entire instrument. Of note, in 1 study utilizing the PHQ-2 in PPD, the instrument performed poorly among economically disadvantaged, multiethnic mothers seeking pediatric primary care in an urban setting, and the authors recommended caution if using in this population and to consider lowering the screen positive threshold.19
Sometimes the issue of medical-legal risks arises when considering implementing screening for maternal depression in pediatric offices. However, there is a strong ethical case in support of implementation of validated screening tools to identify mothers at risk of PPD as early as possible to optimize outcomes for mother and baby.20
Next steps after a positive depression screen
The next steps will depend on the severity of the mother's symptoms, and they range from reassurance to supportive strategies or referral. With milder symptoms associated with postpartum blues, demystification and parent education may be sufficient.
Demystification involves educating the mother that:12,21
· She is not alone.
· She is not to blame.
· She will get better.
Combined with close follow-up, support may be all that is needed. Special attention should be payed to promotion and encouragement of breastfeeding because PPD is associated with discontinuation of breastfeeding.12
If symptoms for mild or moderate depression require further intervention, the pediatrician should provide resources and information on possible treatments. Psychotherapy is effective and considered a first-line treatment. Interpersonal therapy, cognitive behavioral therapy, and psychodynamic psychotherapy (nondirective therapy) all have demonstrated similar effectiveness in the treatment of PPD. Psychotherapy and behavioral therapy also have the benefit of not impacting the breastfeeding mother.2
Pharmacologic management is beyond the scope of this article, but mothers may be referred to their obstetricians, primary care physician (PCP), or to a mental health provider. Few pediatricians provide medical management for mothers’ PPD.22 However, it is important for the pediatrician to communicate with the mother’s obstetrician/gynecologist or PCP and relay symptoms and impressions from the office visit.23
Postpartum depression is a significant problem for families with newborns. Given the long-term impacts of untreated PPD, pediatricians need to be cognizant of its symptoms, provide basic counseling and treatment, and refer for appropriate services when needed.
References:
1. Earls MF: Committee on Psychosocial Aspects of Child and Family Health, American Academy of Pediatrics. Incorporating recognition and management of perinatal and postpartum depression into pediatric practice. Pediatrics. 2010;126(5):1032-1039.
2. Sriraman NK, Pham DQ, Kumar R. Postpartum depression: what do pediatricians need to know? Pediatr Rev. 2017;38(12):541-551. Erratum in: Pediatr Rev. 2018.
3. Silverman ME, Reichenberg A, Savitz DA, et al. The risk factors for postpartum depression: a population-based study. Depress Anxiety. 2017;34(2):178-187.
4. O'Hara MW, Wisner KL. Perinatal mental illness: definition, description, and aetiology. Best Pract Res Clin Obstet Gynaecol. 2014;28(1):3-12.
5. Nelson DB, Freeman MP, Johnson NL, McIntire DD, Leveno KJ. A prospective study of postpartum depression in 17,648 parturients. J Matern Fetal Neonatal Med. 2013;26(12):1155-1161.
6. Kimmel M, Hess E, Roy PS, et al. Family history, not lack of medication use, is associated with the development of postpartum depression in a high-risk sample. Arch Womens Ment Health. 2015;18(1):113-121.
7. Alvarez-Segura M, Garcia-Esteve L, Torres A, et al. Are women with a history of abuse more vulnerable to perinatal depressive symptoms? A systematic review. Arch Womens Ment Health. 2014;17(5):343-357.
8. Paulson JF, Dauber S, Leiferman JA. Individual and combined effects of postpartum depression in mothers and fathers on parenting behavior. Pediatrics. 2006;118(2):659-668.
9. McLearn KT, Minkovitz CS, Strobino DM, Marks E, Hou W. Maternal depressive symptoms at 2 to 4 months postpartum and early parenting practices. Arch Pediatr Adolesc Med. 2006;160(3):279-284.
10. McLennan JD, Kotelchuck M. Parental prevention practices for young children in the context of maternal depression. Pediatrics. 2000;105(5):1090-1095.
11. Leiferman J. The effect of maternal depressive symptomatology on maternal behaviors associated with child health. Health Educ Behav. 2002;29(5):596-607.
12. Kerker BD, Storfer-Isser A, Stein RE, et al. Identifying maternal depression in pediatric primary care: changes over a decade. J Dev Behav Pediatr. 2016;37(2):113-120.
13. Olson AL, Dietrich AJ, Prazar G, Hurley J. Brief maternal depression screening at well-child visits. Pediatrics. 2006;118(1):207-216.
14. Pereira AT, Soares MJ, Bos S, et al. Why should we screen for perinatal depression? Ten reasons to do it. Int J Clin Neurosci Ment Health. 2014;1:10. Available at: https://pdfs.semanticscholar.org/2415/6238ac2984c4b49df9c6477fbbc348c57d57.pdf. Published June 6, 2014. Accessed August 3, 2018.
15. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150:782-786.
16. Kabir K, Sheeder J, Kelly LS. Identifying postpartum depression: are 3 questions as good as 10? Pediatrics. 2008;122(3):e696-e702.
17. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613.
18. Kroenke K, Spitzer RL, Williams JB. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284-1292.
19. Cutler CB, Legano LA, Dreyer BP, et al. Screening for maternal depression in a low education population using a two-item questionnaire. Arch Womens Ment Health. 2007;10(6):277-283.
20. Gilbert AL, Balio C, Bauer MS. Making the legal and ethical case for universal screening for postpartum mood and anxiety disorders in pediatric primary care. Curr Probl Pediatr Adolesc Health Care. 2017;47(10):267-277.
21. Umylny P, German M. Lantiere A. Treating postpartum mood and anxiety disorders in primary care pediatrics. Curr Probl Pediatr Adolesc Health Care. 2017;47(10):254-266.
22. Olin SS, Kerker B, Stein RE, et al. Can postpartum depression be managed in pediatric primary care? J Womens Health (Larchmt). 2016;25(4):381-390.
23. Bauer NS, Ofner S, Pottenger A, Carroll AE, Downs SM. Follow-up of mothers with suspected postpartum depression from pediatrics clinics. Front Pediatr. 2017;5:212.




























