





Photoclinic: Schizencephaly
The adoptive parents of an 11-month-old infant noticed that their son did not use his right arm as often as the left. Concern for brachial plexus injury was raised. Antenatal, natal, family, and early developmental history were unknown.


The adoptive parents of an 11-month-old infant noticed that their son did not use his right arm as often as the left. Concern for brachial plexus injury was raised. Antenatal, natal, family, and early developmental history were unknown.
Physical examination revealed that the infant had left hemiparesis and a head circumference in the sec- ond percentile.Increased tone was noted in his left upper and lower extremities. However, he had good head control and could crawl and maintain a good sitting position. Fine-motor movement was appropriate on the left. He weighed about 17 lb and was 71 cm long.
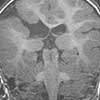
An MRI scan of the brain demonstrated a type II schizencephalic defect along the superior convexity of the right cerebral hemisphere at the level of the posterior body of the right lateral ventricle. This defect affected the posterior frontal and adjacent parietal lobes.
Suzy Mascaro-Walter, MSN, CFNP, and Atiya Khan, MD, of Morgantown, WVa, made the diagnosis of schizencephaly, which accounts for 5% of all cortical malformations in pediatric patients.1 This structural abnormality is characterized by a congenital cleft that crosses the cerebral hemisphere from the pial surface to the lateral ventricles.2 Clefts typically develop in the region of the rolandic and sylvian fissures and involve the frontal cortex; however, they can involve the prefrontal and, rarely, the temporal and occipital lobes. Defects in the walls of the clefts of the cortical plate (eg, thick, microgyric cortex with large neuronal heterotopias) are consistent with migrational abnormalities and are thought to occur in the third month of gestation.
Type I (closed lip) schizencephaly is diagnosed when the walls of the cleft are in contact with each other. Type II (open lip) schizencephaly is characterized by separated lips with cerebrospinal fluid-filled clefts.
Schizencephaly can be unilateral or bilateral. It may present as an isolated malformation or it may be associated with other brain abnormalities, including heterotopia, agenesis of the corpus callosum and septum pellucidum, and septooptic dysplasia. Hydrocephalus can occur with type II schizencephaly.
The cause is likely multifactorial and includes fetal ischemic injury in the middle cerebral artery, mutations in the homeobox gene EMX2 (which is involved in the development of the forebrain), intrauterine Cytomegalovirus infection, and toxins (ie, prenatal drug exposure).3-6 Schizencephaly may be detected early on ultrasonography; it is demonstrated by focal ventricular dilatation. However, MRI is considered the most sensitive test for the identification of migrational disturbances.5
Clinical manifestations include mental retardation, cognitive and language disturbances, motor deficits, seizures (which may not begin until adulthood), and hydrocephalus (open lip lesions). Severity depends on the type, location, and size of the clefts as well as any associated brain malformations. The most severe presentations are associated with large bilateral open lip clefts; the mildest forms are seen with small unilateral closed lip clefts.
Supportive care involves careful monitoring for potential motor and speech delays and for behaviors consistent with seizures. This child exhibits mild cognitive delays; no seizure activity has been reported. He continues to be observed by physical, occupational, and speech therapists.
References:
REFERENCES:
1.
Leventer RJ, Phelan EM, Coleman LT, et al. Clinical and imaging features of cortical malformations in childhood.
Neurology.
1999;53:715-722.
2.
Barkovich AJ, Gressens P, Evrard P. Formation, maturation, and disorders of brain neocortex.
Am J Neuroradiol.
1992;13:423-446.
3.
Dominguez R, Aguirre Vila-Coro A, Slopis JM, Bohan TP. Brain and ocular abnormalities in infants with in utero exposure to cocaine and other street drugs.
Am J Dis Child.
1991;145:688-695.
4.
Granata T, Farina L, Faiella A, et al. Familial schizencephaly associated with
EMX2
mutation.
Neurology.
1997;48:1403-1406.
5.
Barkovich AJ, Kjos BO. Schizencephaly: correlation of clinical findings with MR characteristics.
Am J Neuroradiol.
1992;13:85-94.
6.
Iannetti P, Nigro G, Spalice A, et al. Cytomegalovirus infection and schizencephaly: case reports.
Ann Neurol.
1998;43:123-127.
















